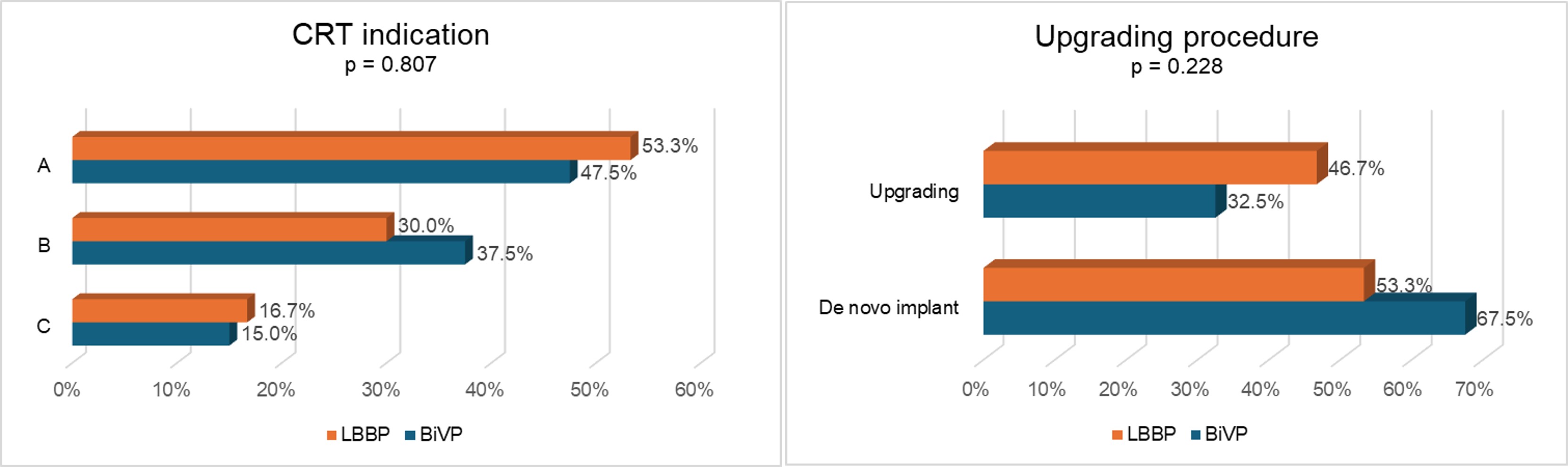
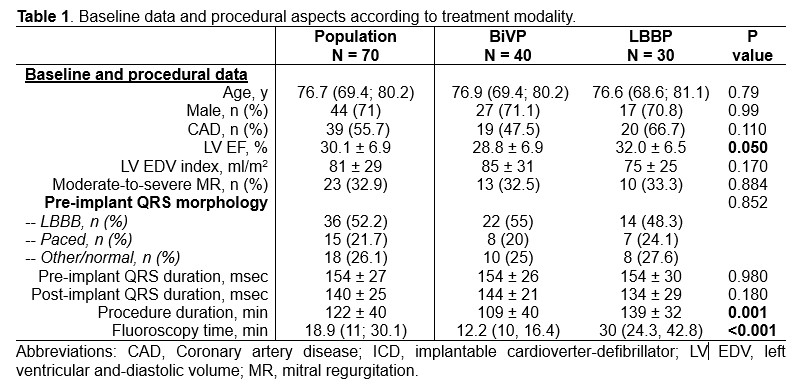
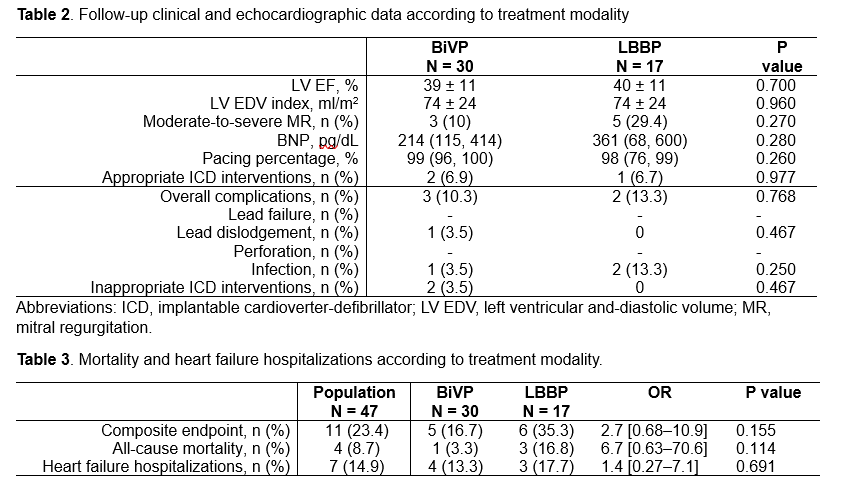
Background: Cardiac resynchronization therapy (CRT) with biventricular pacing (BiVP) is an established treatment for heart failure (HF) with reduced ejection fraction (HFrEF) and wide QRS complexes, is effective in improving outcomes in patients who develop HF as a consequence of right ventricular pacing, and is indicated for patients with mildly reduced left ventricular ejection fraction (LV EF) and high degree atrioventricular block with expected frequent ventricular pacing in order to prevent HF.1–3 Left bundle branch pacing (LBBP) may allow CRT when BiVP is not technically feasible: initial evidence documented non-inferiority of this approach with regard of cardiac remodeling and clinical outcomes.4 Purpose: To describe CRT indications and procedural aspects for different patients’ populations. Methods: This study is a prospective, observational, single-centre registry. Patients with CRT indication (A, HFrEF and wide QRS; B, reduced LV EF and pacing indication; C, pacing-induced cardiomyopathy) who underwent implant procedure between April 2023 and November 2024 were included in the registry. BiVP was the first choice CRT strategy in all cases, while LBBP represented a bailout strategy. Results: Of the 73 patients included in the registry, 40 received BiVP and 30 received LBBP. Three patients received dual- or single-chamber devices and were excluded from this analysis. Median age of the population was 76.4 (68; 80) years, mean ejection fraction was 30±7% (Table 1). Indication for CRT was A in 35 patients (50%), B in 24 patients (34.3%), and C in 11 patients (15.7%). Indications distribution was not significantly different between BiVP and LBBP group (Figure 1). Procedure duration and fluoroscopy time were significantly longer in the LBBP group, as expected for a bailout strategy. The two procedures resulted in similar duration paced QRS complex, in contrast with available evidence. Forty-seven patients had at least 3 months (mean 246±120 days) complete follow-up (Table 2). Clinical and echocardiographic follow-up data were not significantly different between the two groups (Table 2). Complications, mortality and heart failure hospitalizations incidence was not significantly different between the two groups (Table 3). Conclusion: In this HF population, LBBP represents a valid bailout strategy for a wide spectrum of CRT indications when BiVP is not technically feasible, without increasing complications rate.