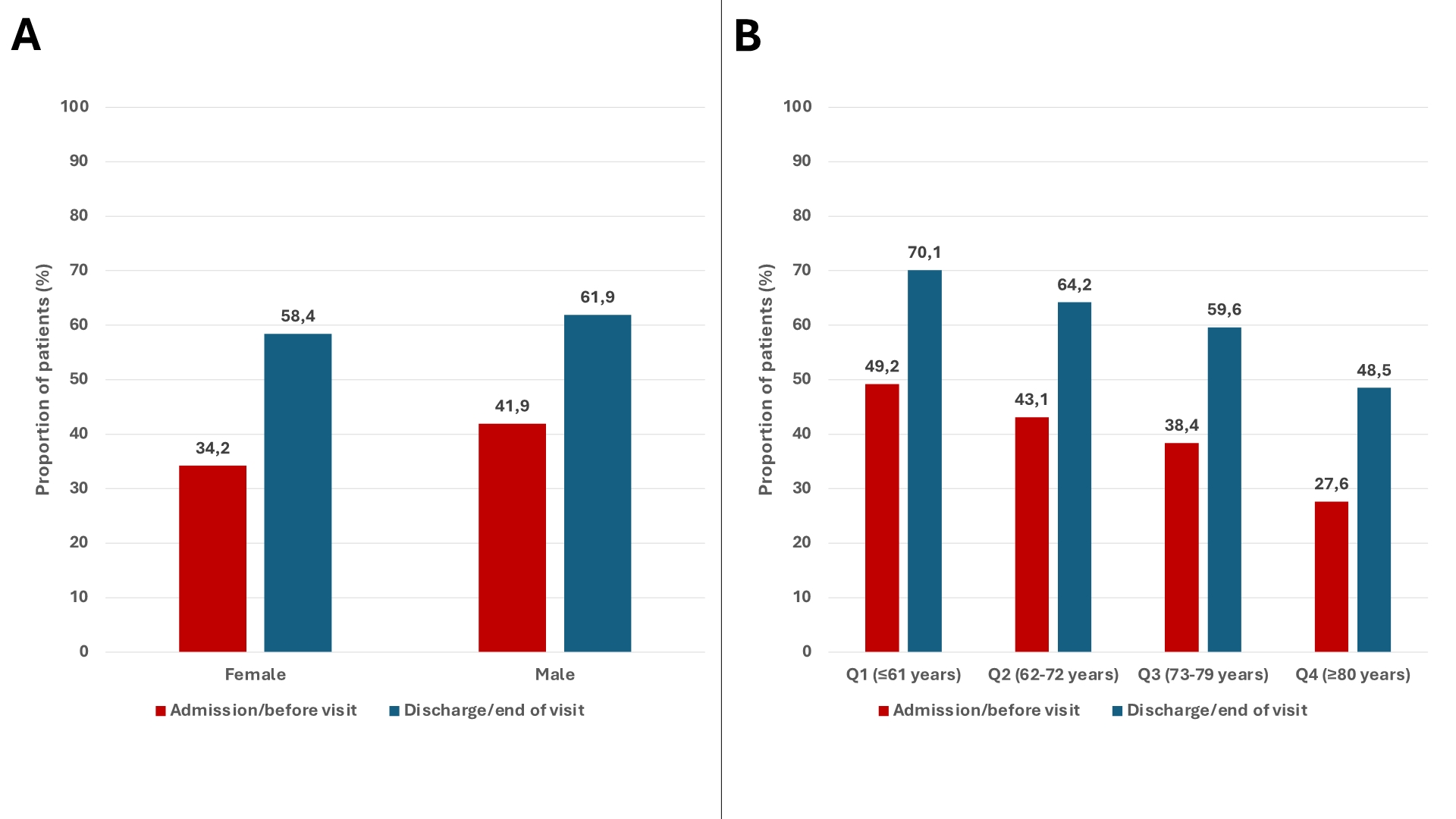
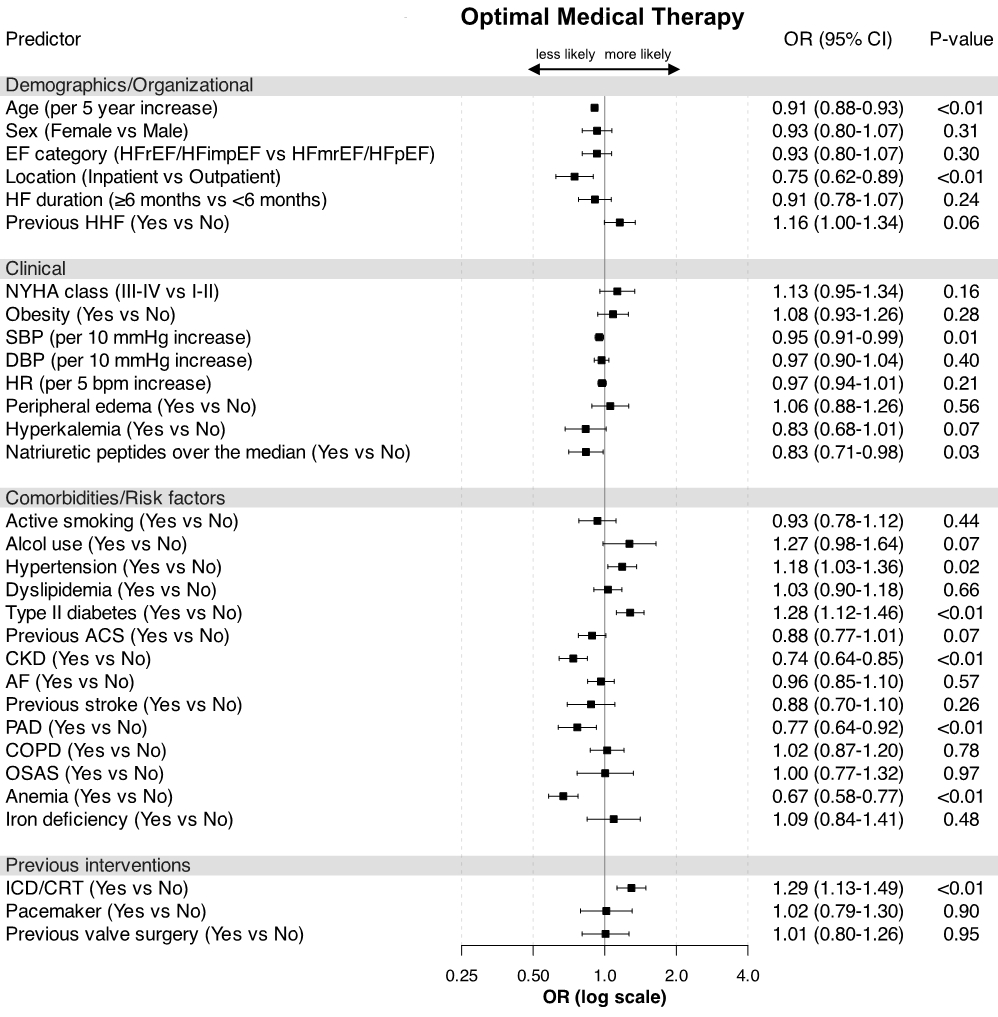
Introduction: Older adults and females are under-represented in randomized clinical trials, and evidence on age – and sex-related differences in heart failure (HF) characteristics and treatment patterns is limited. Purpose: To evaluate differences in the clinical characteristics and treatments of an all-comers cohort of HF patients stratified by age and sex, in a nationwide Italian observational cohort. Methods: The BRING-UP-3 HF study is a prospective, observational, multicenter investigation encompassing 179 Italian cardiology sites. It included an educational intervention for the investigators followed by two three-month enrollment phases and subsequent 6- and 12-month follow-up periods. Optimal medical therapy (OMT) was defined according to the European Society of Cardiology HF guidelines. Multivariable logistic regression models were applied to evaluate predictors of HF treatments across sex and age strata. Results: A total of 5,203 HF patients (median age 72 years; 24% female) were included over 3 months in the first enrollment period. Females were older, had a higher prevalence of non-ischemic HF etiologies, and were less likely to receive guideline-directed medical therapy (GDMT) compared with males. Similarly, older patients also experienced suboptimal treatment, with age being independently associated with a lower likelihood of receiving recommended HF therapies. After multivariable adjustment, female patients were more likely to receive ACE inhibitors/angiotensin receptor blockers (odds ratio [OR] 1.38, 95% confidence interval [CI] 1.13-1.69) and less likely to receive angiotensin receptor/neprilysin inhibitors (OR 0.90, 95% CI 0.86-0.93), with no significant association for other GDMT. Older age was associated with a lower likelihood of receiving all HF GDMT after multivariable adjustment. Outpatient visits and hospitalization represented an opportunity to improve GDMT use, with a significant increase in OMT (Figure 1). After multivariable adjustment, OMT was similarly achieved regardless of sex or EF phenotype, but older patients were still less likely to receive OMT compared with younger patients (Figure 2). Conclusions: Significant age- and sex-related disparities exist in HF characteristics and treatment patterns. Tailored management strategies are needed to optimize GDMT use, particularly for females and older adults, to improve HF outcomes and ensure equitable care.