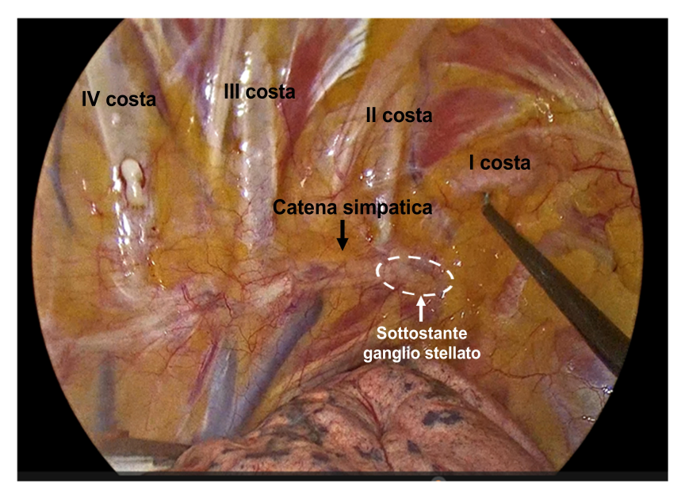
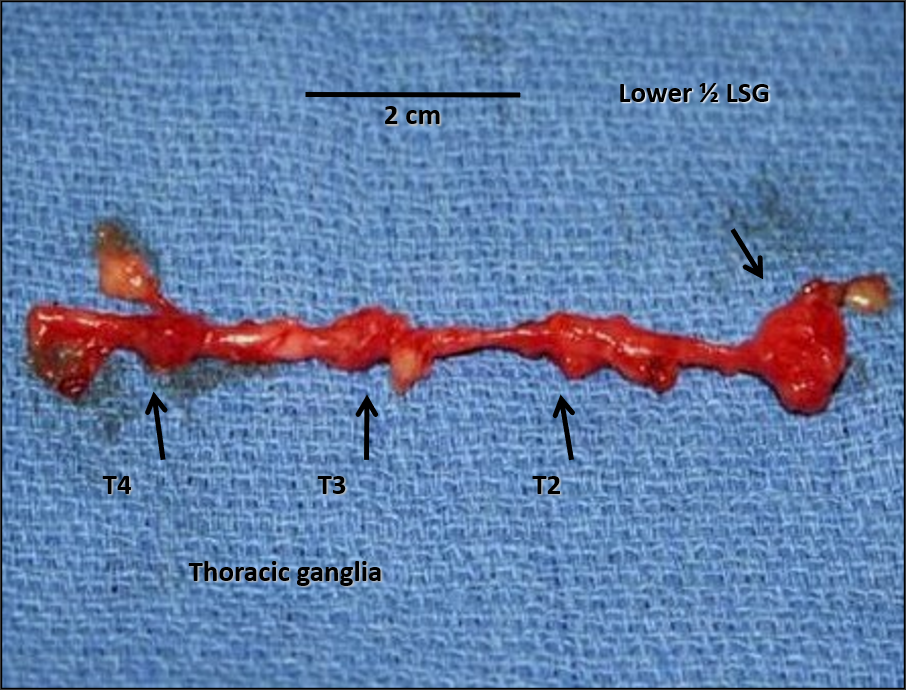
INTRODUCTION: Arrhythmogenic cardiomyopathy (AC) refers to a broad spectrum of phenotypes caused by different genotypes, with in common a high susceptibility to life-threatening ventricular arrhythmias (VAs). Sudden cardiac death may occur even among ICD recipients in case of refractory electrical storm (ES) and/or end of treatment (EOT) condition (exhaustion of ICD therapies either within the same episode or due to low battery). Neuromodulation techniques such as percutaneous left stellate ganglion block (PLSGB) and cardiac sympathetic denervation (CSD) may prevent these conditions by breaking the vicious circle of sympathetic activation. CASE: male, 63 years old, affected by AC with predominant left ventricle involvement, who previously underwent single lead ICD implantation and three transcatheter ablation procedures (the last endo-epicardial) for drug refractory VAs. One night he experienced several syncopal episodes and ICD shocks, and finally a cardiac arrest while driving; upon emergency operators’ arrival, he received four additional external DC shocks. Then he was intubated and transferred to the emergency department of our hospital, where, despite amiodarone drip, he suffered two more episodes of polymorphic VAs (pVAs) requiring external defibrillation. ICD interrogation (Biotronik brand) revealed an EOT condition due to battery depletion, and, previously, 48 episodes of pVAs in VF zone with a total of 92 ICD shocks delivered. In two cases, the maximum number of ICD shocks per episode (8 in the VF zone), was reached, leading to another form of EOT. To acutely stabilize the patient, ultrasound guided PLSGB was performed with ropivacaine 100 mg + lidocaine 100 mg, with no more VAs. The patient subsequently underwent ICD replacement with concomitant upgrading to a dual lead device and, to prevent clustered VAs and future EOT conditions, also thoracoscopic video-assisted bilateral CSD, without complications. No further recurrences have occurred at seven months follow-up. CONCLUSION: In specific circumstances such as AC where the substrate is continuously evolving as well as the underlying autonomic dysfunction, a focal therapy such as VT ablation, despite acutely effective, might not be enough to prevent recurrences from new arrhythmic foci and/or due to pVAs, even in form of deadly ES among ICD recipients. Cardiac neuromodulation carries a particularly strong rationale in this setting and should be considered earlier in patients’ management.