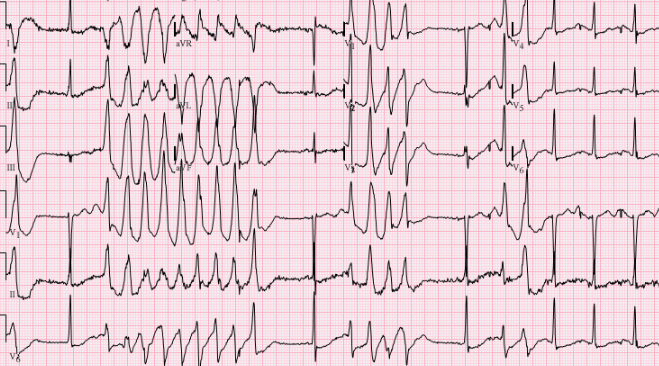
Background It is known that QT and QTc interval prolongation can cause life-long malignant arrhythmias. Even severe alterations in serum electrolytes, although reversible, can in some subjects unmask some mutations present in heterozygosis and therefore generally well tolerated. However, it is not possible to associate any mutation with a certain number of arrhythmias, perhaps because they have not yet been identified or are too rare to constitute a clear indication for treatment. Clinical case A 38-year-old female patient experienced three syncope during last 24 Hours. At Emergency Department she had psychomotor agitation treated with benzodiazepines. The ECG was unremarcable with normal QT and QTc but at continous monitorig ecg shown ventricular tachycardia and torse de point. The blood test shown normal cells count and very low K 2.8 mEq/l,. The patient was transferred to the cardiology intensive care unit where further blood tests shown elevated level aldosterone and renina with norml urniray iones and persistent very low potassium 2.9 mEq/l; she treated with idratation and potassium EV. She was then subjected to an echocardiogram which showed normal diameters of the cardiac chambers, normal thicknesses and normal ejection fraction of the left ventricle and a heart MRI which undoubtedly showed minor morphological alterations of the mediobasal lateral wall of the right ventricle. The patient also underwent an endocrinological and nephrological consultation for suspected Bartter syndrome. The classic genetic testings for long QT syndrome, were negative, but in the CNR study showed a heterozygous mutation of the AKAP9 which encoding a potassium channel-associated kinase A anchoring protein. The patient was discharged after S-ICD implantation. At the follow-up visit she was fine and without any more syncope. Conclusion The most interesting aspect in this case is that even genetic alterations of currently uncertain significance can, in conditions for other causes of plasma electrolytes, be associated with malignant and life-threatening arrhythmias. It is therefore, in our opinion, advisable to perform genetic tests where basic research is being carried out. BIBLIOGRAPHY Protein Kinase A Regulates Platelet Phosphodiesterase 3A through an A-Kinase Anchoring Protein Dependent Manner. Jawad S Khalil et al. Cells. 2024 Jun 26;13(13):1104 European Heart Journal, Volume 43, Issue 40, 21 October 2022, Pages 3997–4126