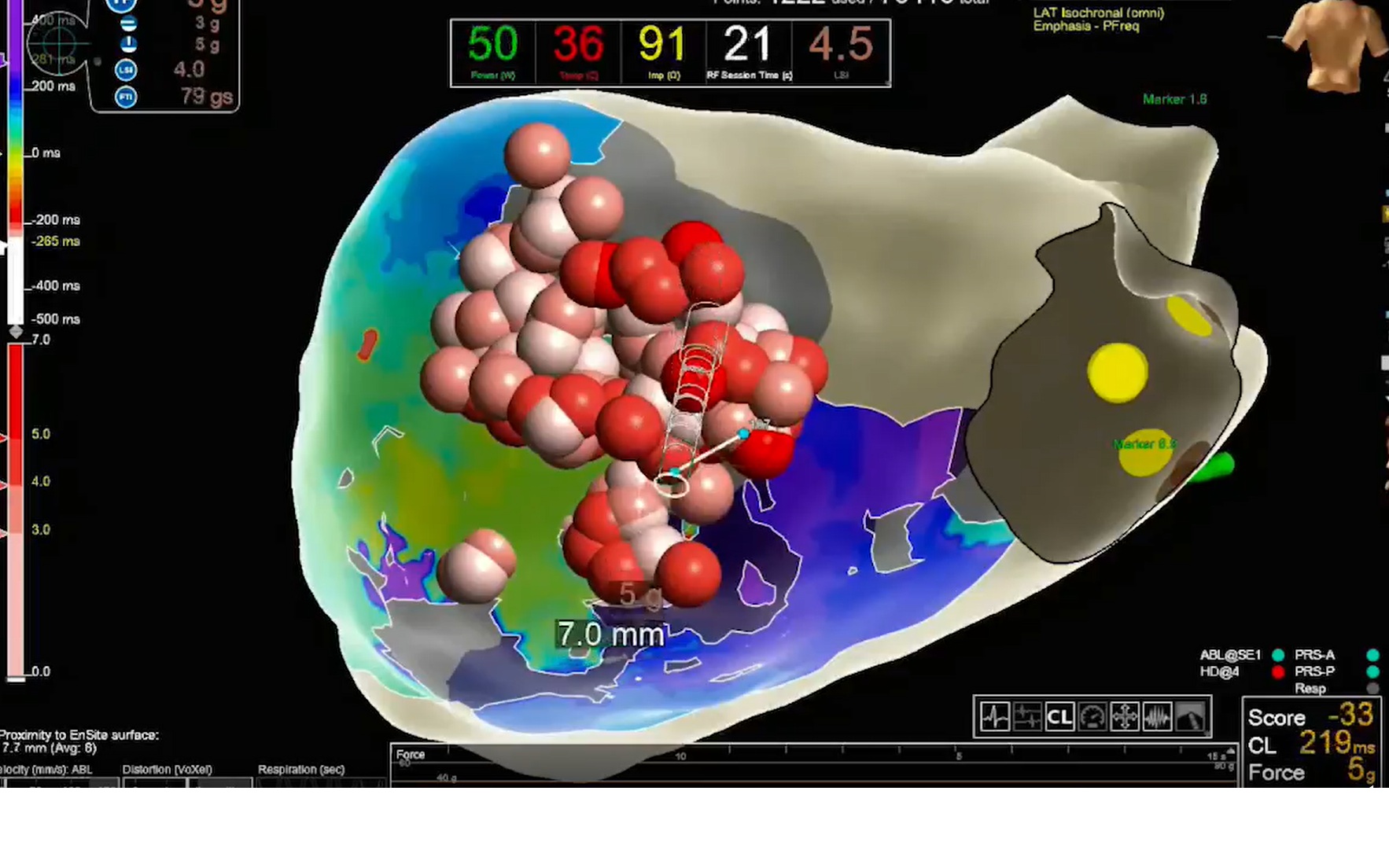
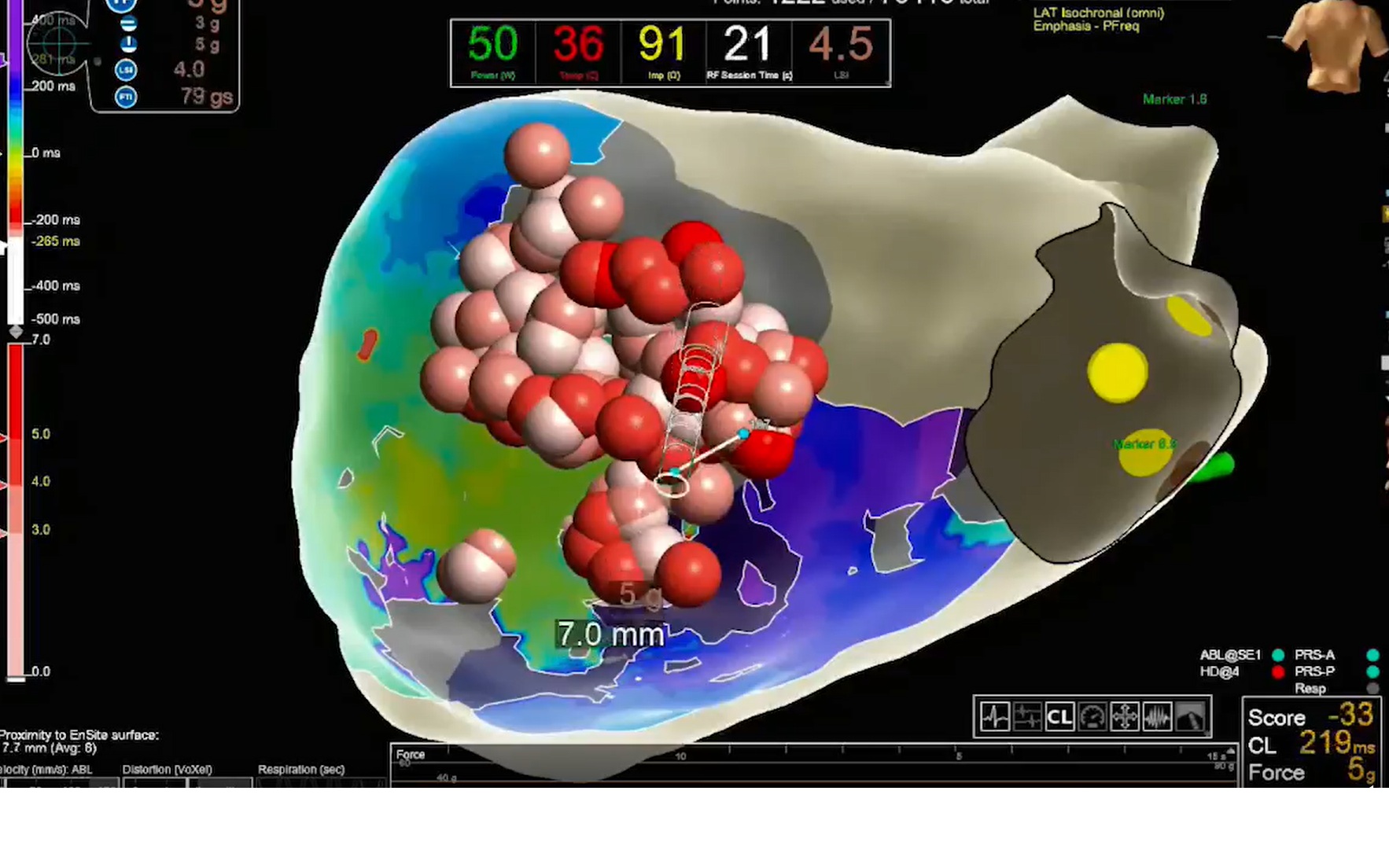
A 74-year-old woman with a history of hypertension, diabetes, and ischemic heart disease was admitted to the hospital following the acute onset of palpitations. She had an ICD implanted 5 years earlier for primary prevention of sudden cardiac death due to ischemic cardiomyopathy with reduced left ventricular ejection fraction (LVEF 30%) and a previous inferior myocardial infarction. Upon arrival, the patient was in severe distress, with a heart rate exceeding 200 beats per minute. Her ICD had delivered 30 episodes of antitachycardia pacing (ATP) over the previous 24 hours in an attempt to control the arrhythmias, resulting in “electrical storm”. A coronary angiography revealed no significant coronary artery stenosis or acute occlusions. The patient was started on a combination of antiarrhythmic medications, including amiodarone, metoprolol, lidocaine, magnesium, and dexmedetomidine. Despite these efforts, the patient’s VT episodes persisted, and her condition remained critical. Given the failure of medical management and the persistence of electrical storm, a left percutaneous stellate ganglion block was performed. The procedure, which involves injecting a local anesthetic near the stellate ganglion, resulted in an immediate reduction in arrhythmic burden and a noticeable improvement in her hemodynamic status. To further understand the arrhythmogenic substrate, an electrophysiological study was conducted. The study revealed a wide aneurysmatic region in the inferior wall of the left ventricle, which was identified as the primary substrate for the arrhythmias. Late activation areas (LAVA) were observed in the border zone of the aneurysm, confirming the presence of a critical arrhythmic substrate. Based on the electrophysiological mapping, a targeted VT ablation was performed. The procedure involved radiofrequency ablation of the areas of late activation, particularly in the border zone of the aneurysmatic inferior wall. Successful ablation was achieved, with the elimination of the arrhythmogenic substrate. After the procedure, no further episodes of electrical storm were noted, and the patient’s ICD was reprogrammed to minimize the need for ATP therapies. The patient was gradually weaned off intravenous medications, and her clinical condition stabilized. The patient was discharged after 10 days in stable condition and continued to follow up in the outpatient clinic. At her 6-month follow-up, the patient remained free from recurrent VT or electrical storm.