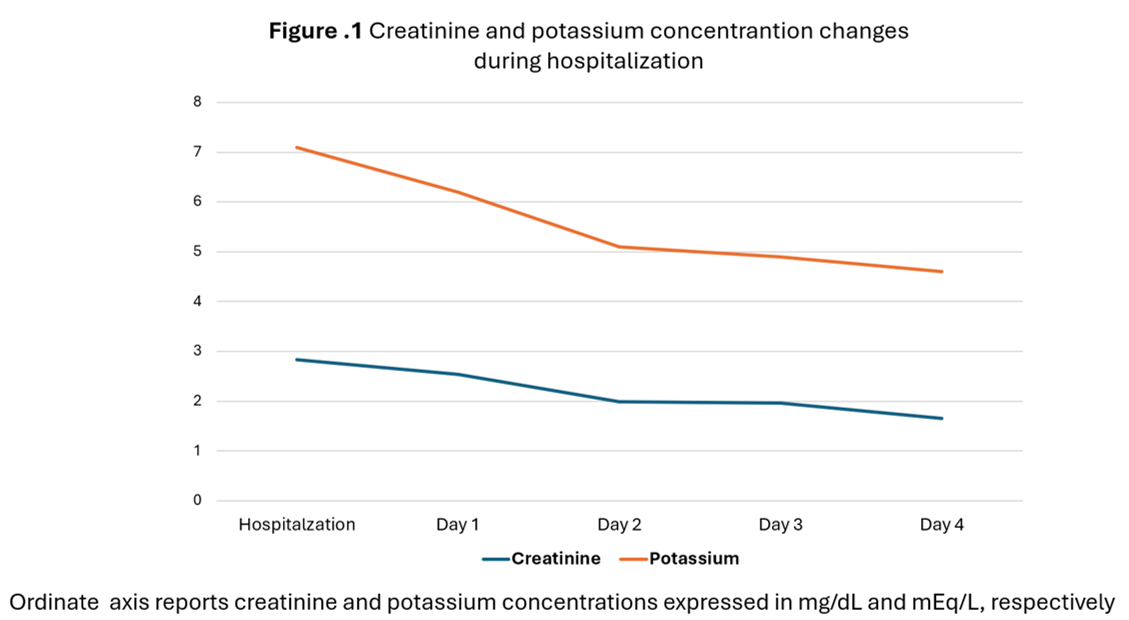
Background. Bempedoic acid is an established treatment for dyslipidemia. In randomized clinical trial the treatment with bempedoic acid was associated with a small increase in creatinine levels. We present the case of a patient with chronic coronary syndrome, heart failure with mild reduction of ejection fraction, and dyslipidemia with statin intolerance, The patient was treated with ezetimibe, PCSK9 monoclonal anti-body, bempedoic acid, mineral receptor antagonists (MRAs), gliflozins, and angiotensin receptor blockers (ARBs) and developed acute kidney function impairment which promptly resolved with drugs withdrawn and hydration. Case report. A 70-year-old women with history of hypertension, dyslipidemia and previous coronary percutaneous revascularization, statin intolerance treated with ezetimibe, PCSK9 monoclonal anti-body, MRAs, gliflozins, and ARBs presented in an outpatient visit. The patient showed laboratory analysis with C-LDL 78 mg/dl. The renal function and electrolytes levels were normal. To optimize lipid-lowering treatment bempedoic acid 180 mg/die was added. At laboratory analysis control scheduled after one month of treatment high creatinine levels (2.63 mg/dl) and hyperkaliemia (6.3 mEq/L) were found. The patient was hospitalized, and hydration therapy and sodium polystyrene sulfonate were immediately started. Furthermore, at hospitalization MRAs, gliflozins, and ARBs were withdrawn. Kidney and urinary tracts ultrasound and renal arterial Doppler examination performed during hospitalization did not show anything of relevant. Over the hospitalization, laboratory analyses showed a progressive reduction in creatinine and potassium levels (Table 1). Patient treatment prescribed at discharge was: bisoprolol; furosemide, ASA, ezetimibe, and PCSK9-inibitor. Conclusion: This case shows that acute kidney function impairment related to polypharmacy may be promptly resolved with hydration and the withdrawn of drugs potentially linked to creatinine increase.