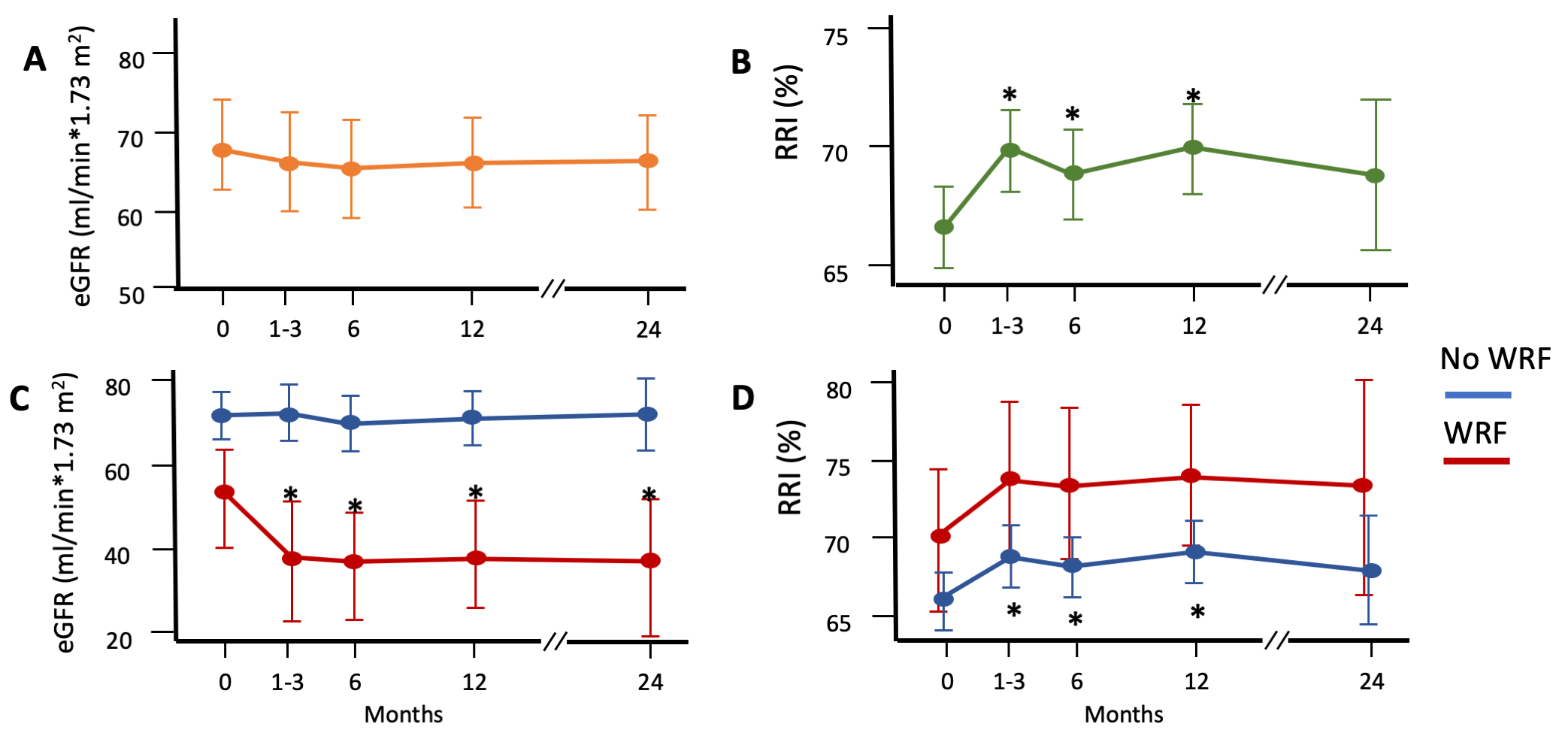
Background. Type 2 sodium glucose cotransporter inhibitors (SGLT2i) have demonstrated cardiorenal protection in patients affected by type 2 diabetes mellitus (T2DM), chronic kidney disease (CKD) and chronic heart failure (CHF). Among the mechanisms underlying this benefit, there is the possible restoration of tubuloglomerular, which contrasts glomerular hyperfiltration and the progression of CKD. Aim of the study. To evaluate the relationship between the introduction of SGLT2i, the estimated glomerular filtration rate (eGFR) and the arterial renal resistance index (RRI) in CHF outpatients with reduced ejection fraction (HFrEF). Methods. Fifty-two patients (mean age 60±13, 81% males, NYHA class 2.2±0.39, 21% with T2DM and 31% with CKD) affected by HFrEF (mean left ventricular ejection fraction, LVEF, 31±7%) and in conventional therapy (100% ACE-inhibitors or ATII receptor antagonists or sacubitril/valsartan, 100% beta-blockers, 86% mineralcorticoid receptor antagonists) were enrolled. Before and 1 or 3, 6, 12, and 24 months after SGLT2i prescription, eGFR by serum creatinine levels and the renal resistance index (RRI) by echo Doppler were evaluated. Changes in the repeated measures were evaluated by linear mixed models. A p<0.05 was considered significant. Results. In comparison with baseline values, a non-significant reduction in eGFR but a significant increase in RRI values was observed at 1-3, 6 and 12 months (see Figure panels A and B). During early follow-up, 13% of patients showed early worsening of renal function (WRF, defined as an increase of serum creatinine > 0.3 mg/dl with an eGFR reduction >25%). Among patients with and without WRF, eGFR diverged, whereas a similar trend in change of RRI was observed. Conclusions. In HFrEF patients, after SGLT2i introduction a significant increase in RRI observed in patients with and without early WRF. These data strengthen the possible effects of SGLT2i on afferent arterioles and hyperfiltration, considering that afferent and efferent arterioles are mainly responsible for renal resistance variations.