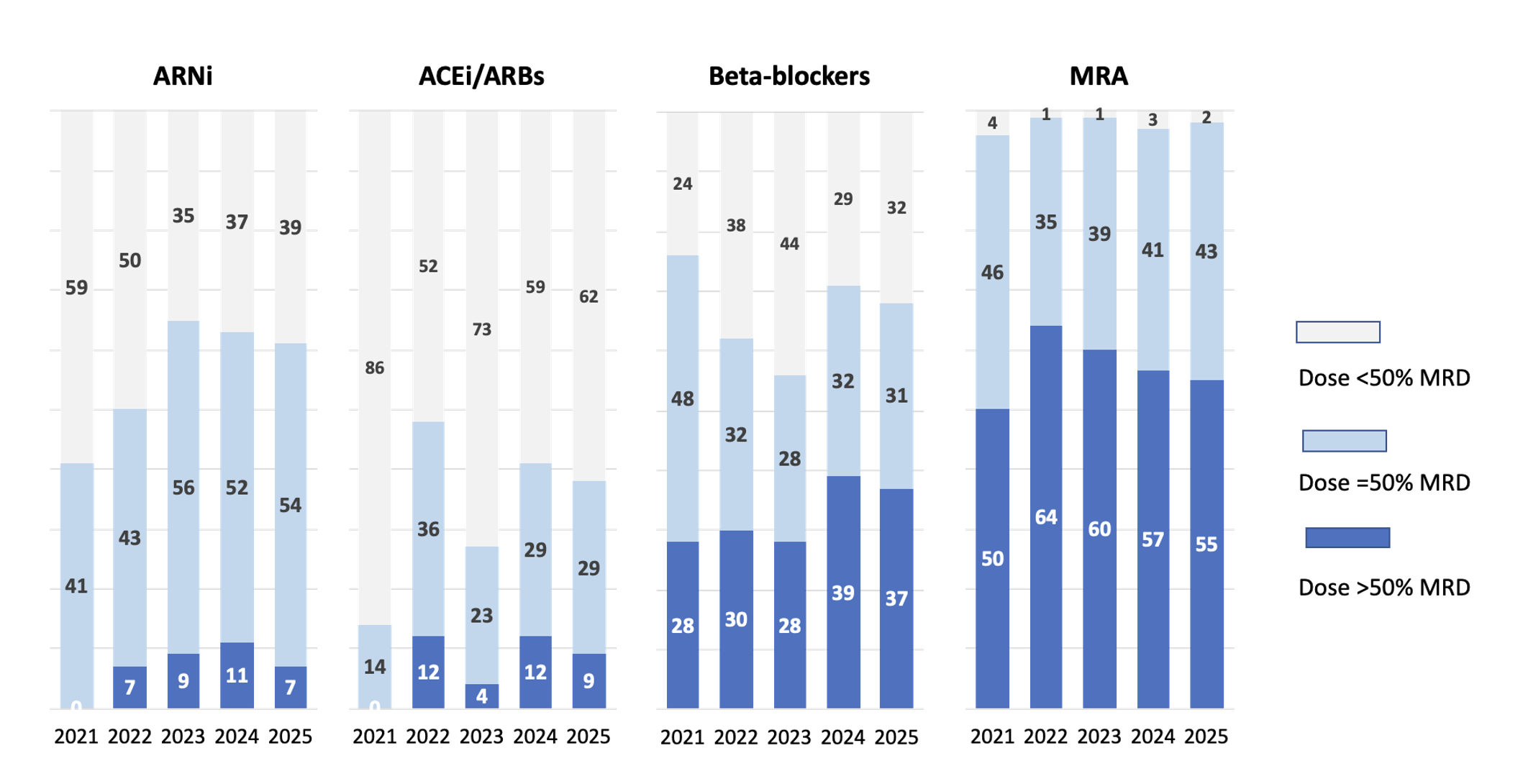
Background & Study Aim. In patients with heart failure with reduced ejection fraction (HFrEF), the use of four main pharmacological classes is currently recommended: angiotensin receptor–neprilysin inhibitors (ARNI), preferred over angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARB), beta-blockers, mineralocorticoid receptor antagonists (MRA), and sodium–glucose co-transporter 2 inhibitors (SGLT2i). The aim of this study was to evaluate trends in prescribed dose adjustments of ACEi/ARB/ARNI, beta-blockers, and MRA over recent years, following the introduction of SGLT2i, in patients enrolled in the PONTE SC/SCA registry. Methods and Results. Among the 496 patients with HFrEF enrolled in the registry, both retrospective (2021–2023) and prospective (2024–2025) analyses were performed. Over this period, prescription rates of ACEi/ARB/ARNI (82–89%), ARNI (58–64%), MRA (84–86%), and beta-blockers (93–96%) remained stable, whereas a significant increase in SGLT2i prescription was observed, from 10% to 85%. The increased use of SGLT2i did not affect the dosing of the other pharmacological classes; however, the proportion of patients receiving the maximum recommended dose remained low, particularly for ARNI and ACEi/ARB (Figure). Conclusions. In the PONTE SC/SCA registry, the increased use of SGLT2i did not influence either prescription rates or dosing of the other recommended drug classes. Nevertheless, these findings highlight the need to increase the proportion of patients treated with ARNI at the maximum recommended dose.