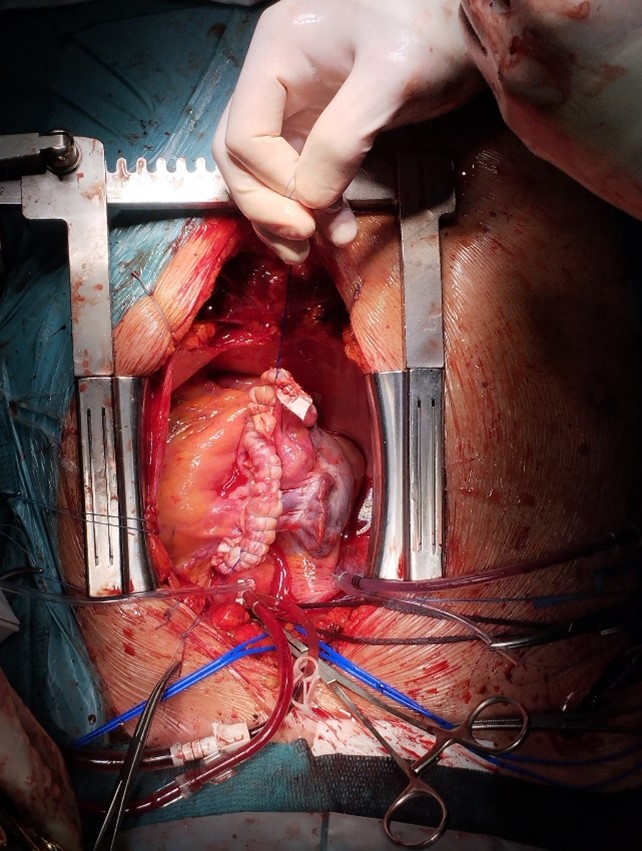
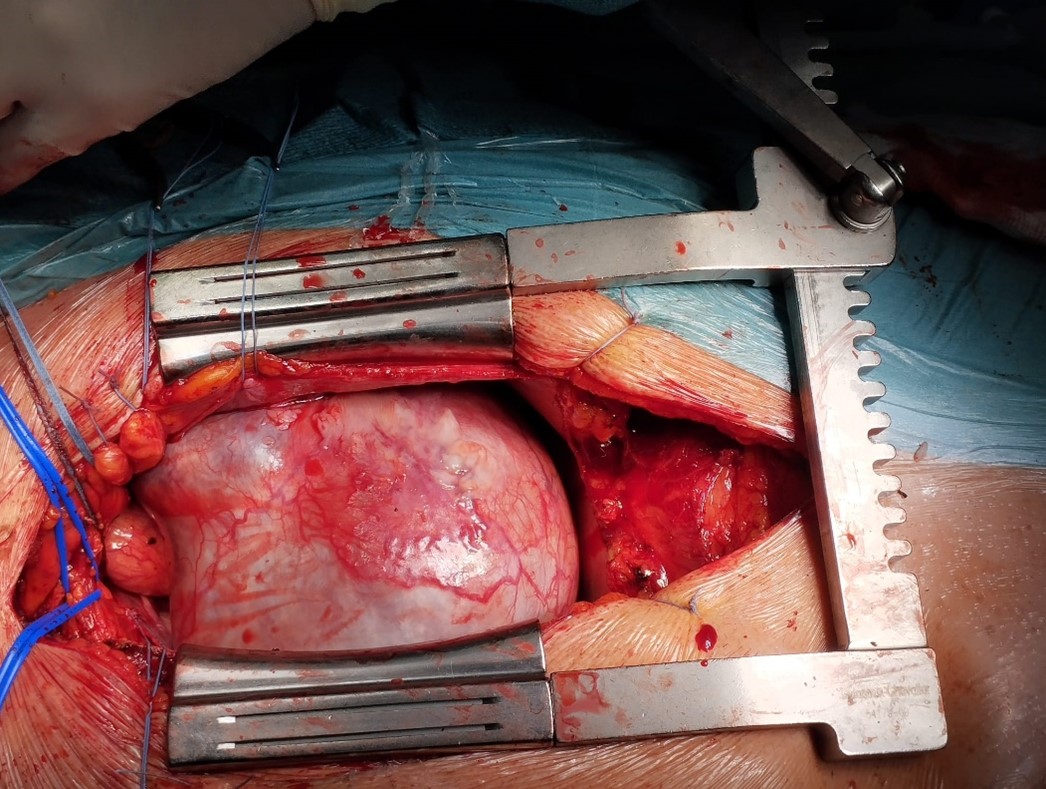
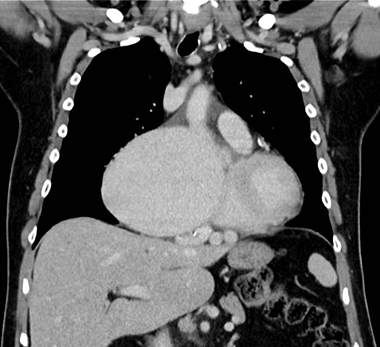
Coronary artery aneurysm is defined as a segment of the artery in which dilation exceeds the diameter of an adjacent portion (considered as a reference point) by more than 1.5 times. In rare circumstances coronary aneursyms can be pointed out as giant, in which the diameter is 4 times the diameter of the reference coronary vessel or is over 8 mm. The pathophysiology of coronary aneurysm development is still uncertain. Atherosclerosis, Kawasaki disease, Takayatsu arteritis and other vasculitic disorders can be a predisposing risk factor in the development of such anatomical anomaly. Symptoms of GCAA include chest pain, shortness of breath, and palpitations. Sometimes patients are asymptomatic. Complications of GCCA include myocardial infarction, thrombosis, and sudden death. Coronary angiography is the gold standard for diagnosis and evaluation of CAAs, but the main limitation of this diagnostic tool is the inability to properly define the dimension of the aneurysm in case of intraluminal thrombi formation, this is why MSCT scan can be exploited as an additional non-invasive imaging technique. Nowadays there is still no agreed consensus on the best strategy to identify and treat the malformation, hence the difficulty in creating an adequate protocol. We recently treated a patient diagnosed with an asymptomatic giant coronary artery aneurysm with the size bigger than a tennis ball. Even if asymptomatic, being the dimensions excessive and the risk of sudden death increased, we opted for a full pre-operative work-up. Pre-operative assessment consisted of coronary angiography, MSCT scan and cardiac US, all of them confirming the suspect of a giant CAA arising from the right coronary artery. We proceeded with surgical excision and ligation of the anurysm in median sternotomy. Post-operative CT scan showed the net reduction in size of the known aneurysm with no evidence of active blood reperfusion to the aneurysmatic remnant. In conclusion, CAAs are rare but potentially catastrophic. Early diagnosis and treatment are pivotal in order to prevent serious complications. Kawasaki disease and Takayatsu arteritis should be excluded during diagnostic work-up, as they can benefit from specific treatments. Nowadays there is still no agreed consensus on the best strategy to identify and treat the malformation (either endoscopically of surgically), hence the difficulty in creating an adequate protocol.