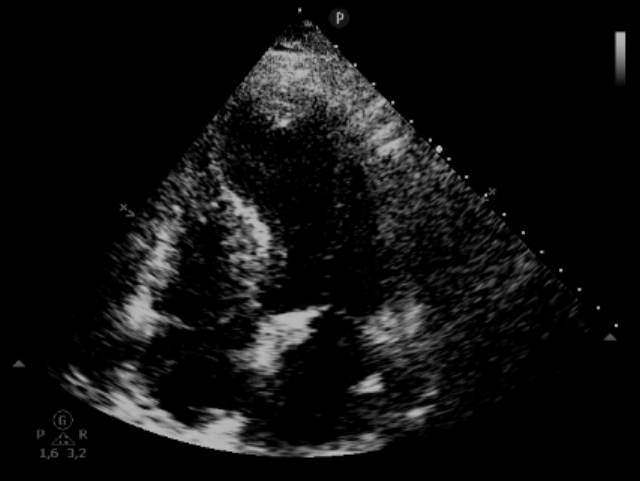
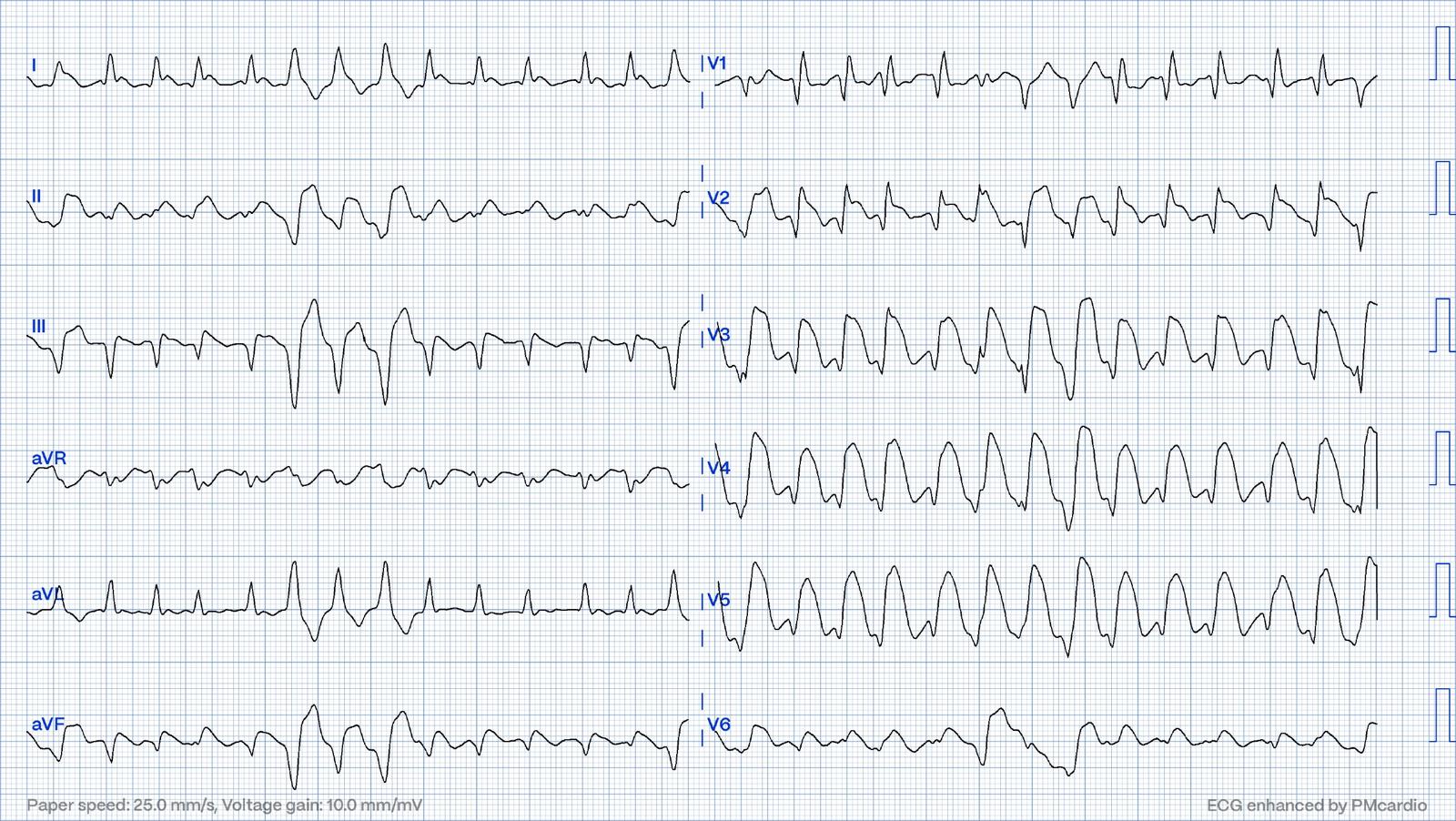
Introduction: Takotsubo Syndrome (TTS) is a condition typically brought on by significant emotional or physical stress. Clinically, it presents with chest pain, electrocardiographic abnormalities, elevated troponin levels and transient regional left ventricular dysfunction that mimics acute myocardial infarction but without evidence of obstructive coronary artery disease or plaque rupture. ST elevation has been described in about 56% of TTC cases, however with amplitude tipically lower than in STEMI. Here we report a case of massive ST elevation, the so-called shark-fin-sign. Case report: a 92-year-old man presented to emergency department complaining about abdominal pain and vomiting with evidence of acalculous cholecystitis. Past medical history included a recent NSTE-ACS due to acute occlusion of RCA treated with pPCI, without left ventricle systolic dysfunction (EF 55%). During the stay in the emergency room, due to new-onset dyspnea and hypotension, an ECG was performed releaving atrial fibrillation with massive anterior ST segment elevation (shark-fin sign). Echo showed severe left ventricle systolic dysfunction (EF 25%) with apical ballooning and thrombus. Prompt coronary angiography revealed good result of previous PTCA on RCA, with no other relevant coronary arterial plaques. The patient was started to dobutamine+noradrenaline due to circulatory shock (both cardiogenic and distributive due to sepsis), antibiotics, intravenous diuretic, unfractionated heparin (UHF) and ventilatory support using CPAP. In the following days clinical conditions slowly improved and seriate echo revealed progressive improvement of LV systolic function (EF 40%), regression of apical ballooning and resolution of apical thrombus. Also ECG showed evolutive signs typical of TTS, with regression of ST segment elevation and appereance of diffuse negative T waves. The patients was discharged home with HFrEF GDMTs, in good clinical conditions. Conclusions: Shark-fin sign is defined as a distinctive, giant triangular R wave (amplitude ≥ 1 mV) resulting from the fusion of the QRS complex, the ST segment and the T‐wave. Despite it has been associated more often with injury due to LAD coronary occlusion, it may also be related to TTS, as recent reports confirm. The presence of this pattern during the acute phase of stress cardiomyopathy appears to be related to a higher risk of adverse events at short and long-term follow-up.