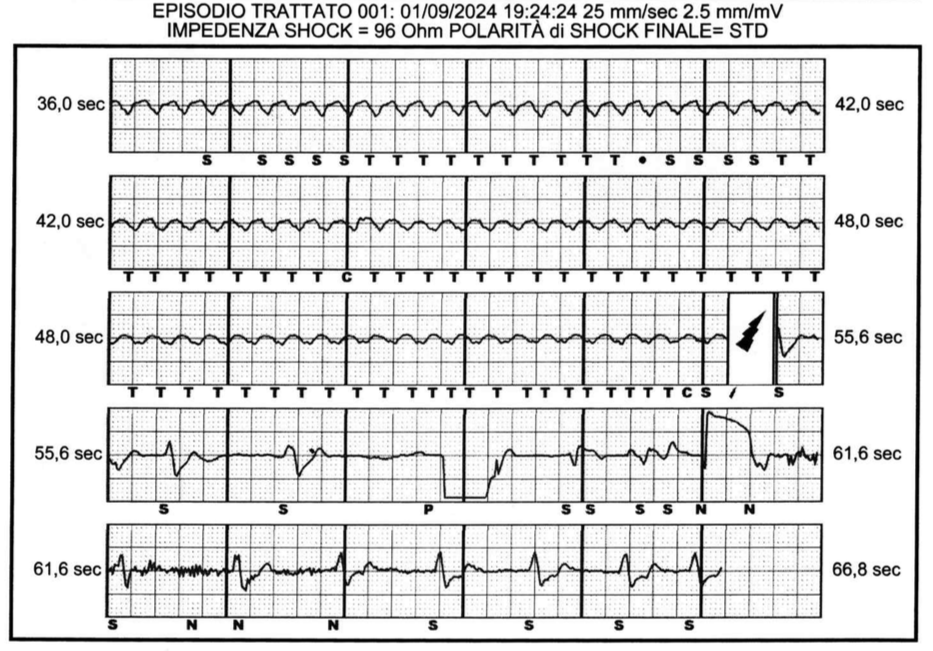
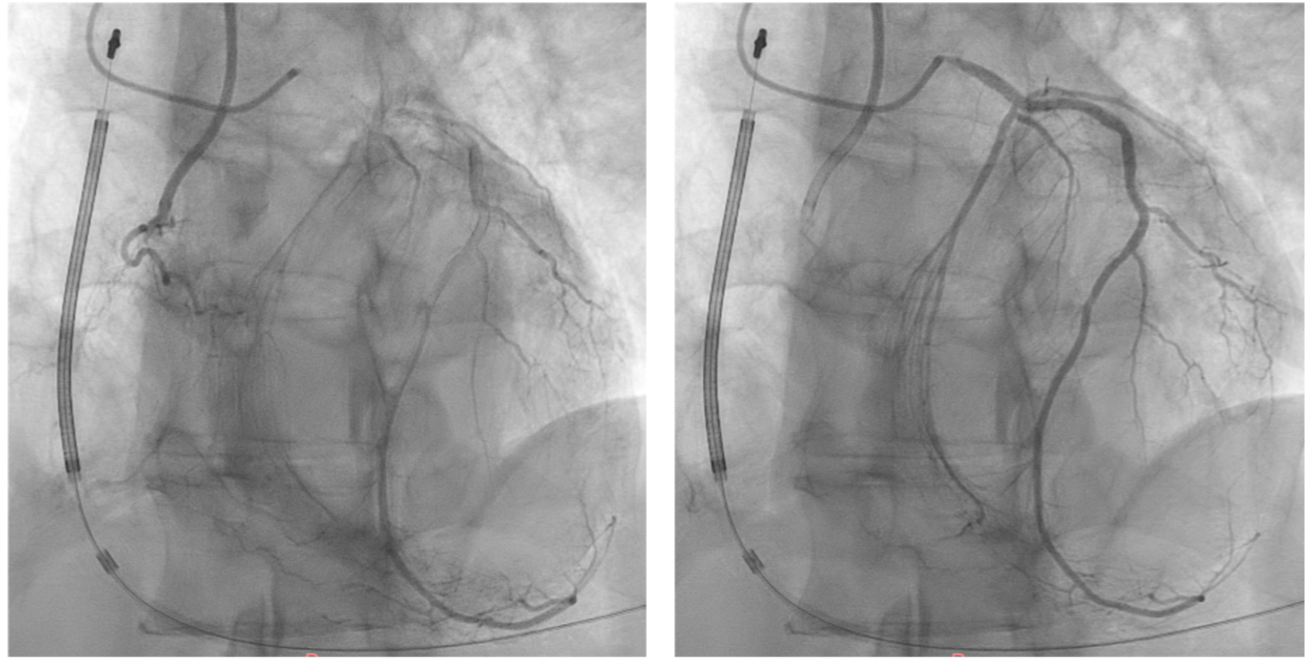
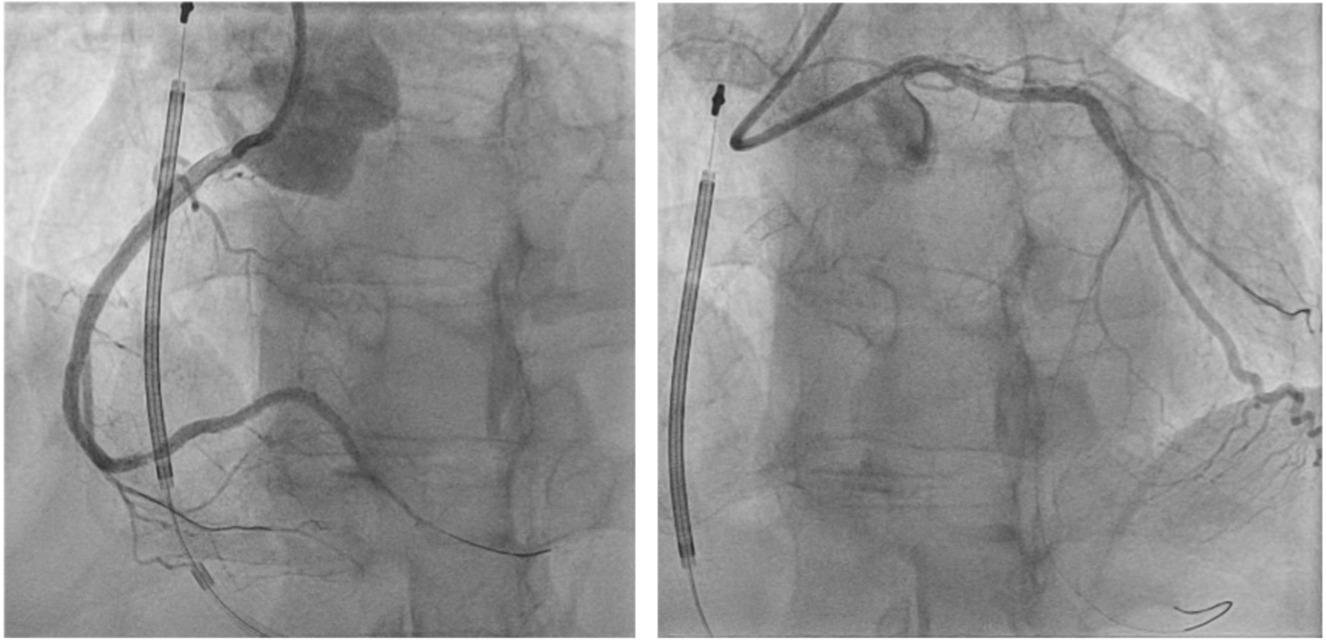
MC is a 55yo and 70kg man, previous smoker, with arterial hypertension, dyslipidemia and family history of coronary artery disease. On January 1st 2024 he came to the Emergency Department for a syncope at home without symptoms: the ECG showed an antero-apical necrosis with severe left systolic dysfunction (LVEF 15%) at the echocardiogram. The subsequent coronary angiography documented RCA total chronic occlusion and LAD severe proximal stenosis treated with PTCA and DES without any complication. The patient was discharged with a wearable ICD and 3 months later, without EF recovery (LVEF 20%) because of dilated LV with IVS, inferior and anterior akinesia and mild-moderate mitral regurgitation, he received a subcutaneous ICD. On September 2024 he came again to ED: severe fatigue interrupted an effort twice and subsequently he lost consciousness. The ECG was normal but cardiac biomarker was elevated (hsTnT basal 43ng/l and at 1h 173 ng/l) so he was admitted to ICU. DAPT, MRA, ARNI, BB and SGLT2i continued. ICD control revealed sustained VT 210bpm treated with ATP ineffective and then with DC shock effective. Amiodarone started and the coronary angiography demonstrated critical stenosis at both LAD proximal and CX and confirmed the RCA chronic total occlusion with heterocirculation. Echocardiogram showed dilated LV with posterior IVS, apex and distal anterior wall akinesia and residual hypokinetic walls conditioning LVEF <30%. We referred the patient to our HUB for advanced therapies: due to young age and severe left ventricular dysfunction, we avoided carrying out the simplest path of complete surgical revascularization by opting for a complex PTCA on the three vessels to leave chance for any subsequent non-conventional treatments (LVAD, Artificial Heart, Cardiac Transplant). Viability test were excluded because of ICD and hard arrhythmic burden so, after mechanical cardiac support positioning, PTCA and DES implant was performed to LAD and anterograde RCA recanalization with PTCA and 4 DES implant was performed, medical therapy for Cx. A femoral pseudoaneurism complicated the procedure but medical therapy was indicated. Contextually the screening for unconventionally heart failure therapies started: OPT, EGDS, colonoscopy and psychological evaluation resulted favorable. The multidisciplinary and interhospital team made it possible to obtain complete revascularization, promptly start screening for advanced HF therapies and avoid early thoracic surgery.