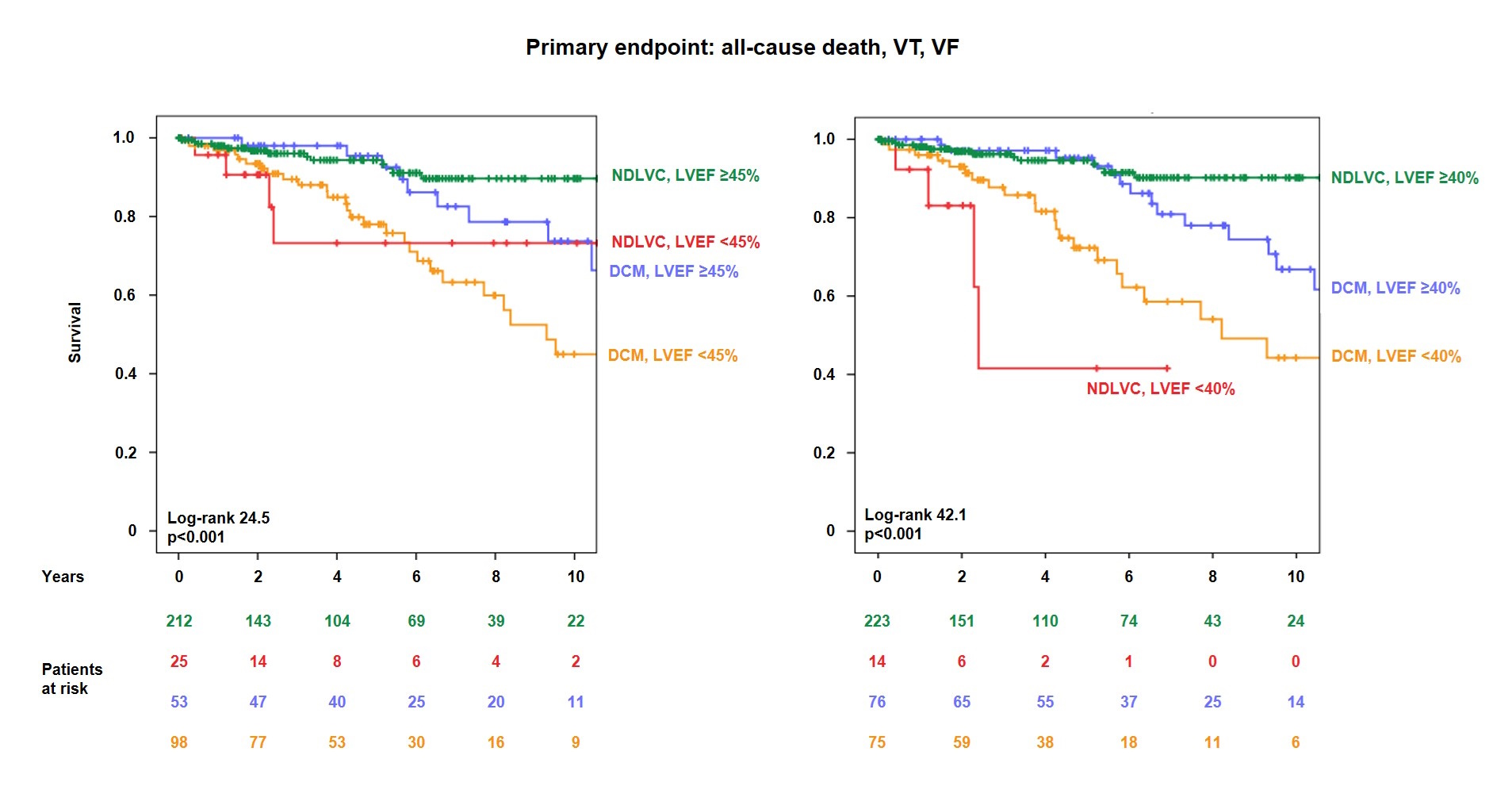
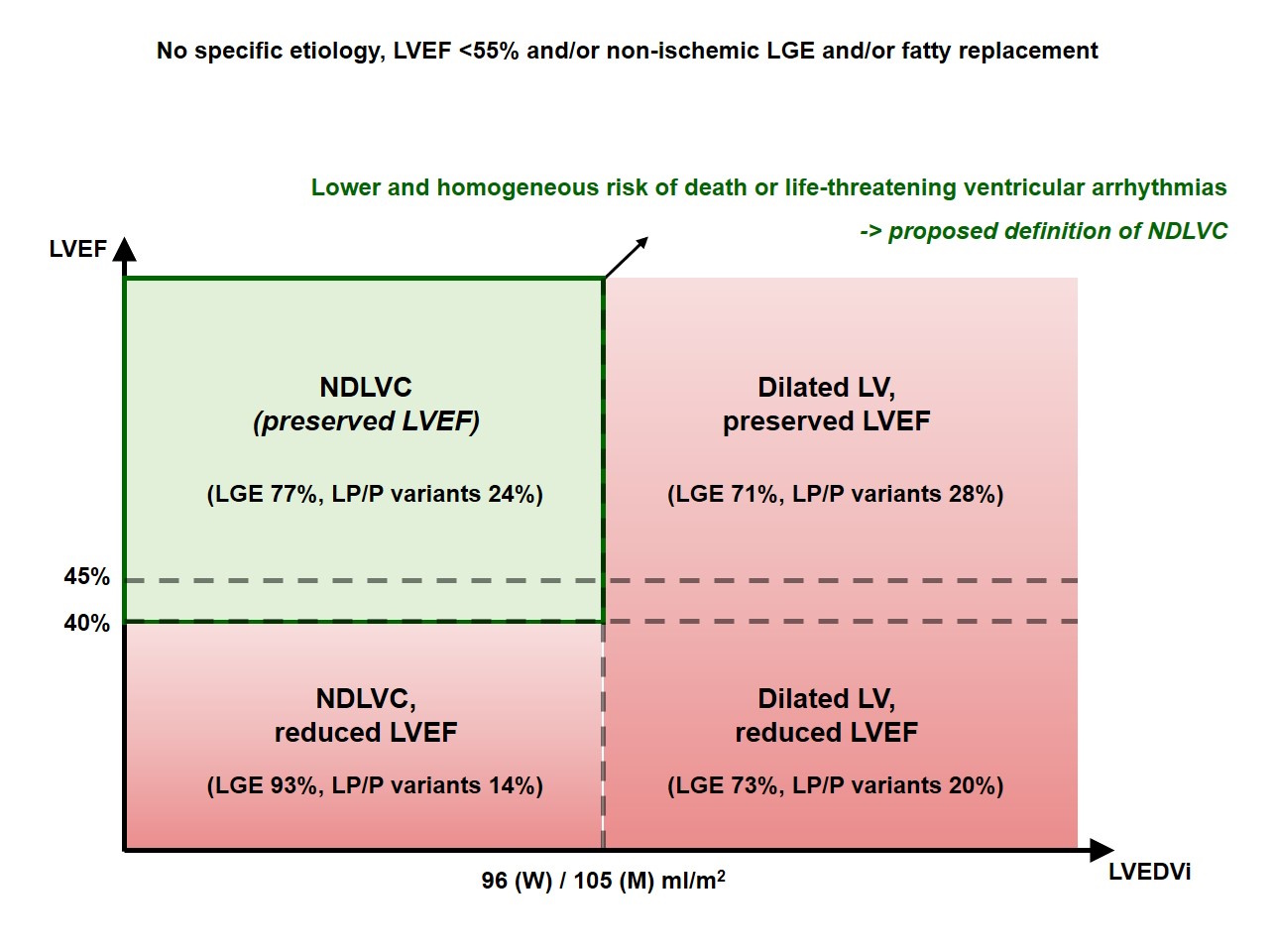
Background: Non-dilated left ventricular cardiomyopathy (NDLVC) has been defined as non-ischemic LV scarring and/or fatty replacement and/or hypokinesia, without LV dilation. This definition omits specific criteria for LV dilation or even dysfunction. Methods: We identified all non-ischemic cardiomyopathy patients undergoing a cardiovascular magnetic resonance scan from 2012 to 2022 with LV ejection fraction (LVEF) <55% and/or non-ischemic late gadolinium enhancement (LGE) and/or fatty replacement. Patients with hypertrophic cardiomyopathy or amyloidosis were excluded. The primary endpoint was a composite of all-cause death, sustained ventricular tachycardia or fibrillation. Results: The cohort included 388 patients (32% women, median age 55 years [interquartile range 43-63]). Over 4.3 years (1.9-7.0), 59 patients (15%) developed a primary endpoint event. The risk increased exponentially with LVEDVi values, with inflection points approaching the upper reference limit of LVEDVi (<96 mL/m2 in women, <105 mL/m2 in men). Using these criteria, we identified NDLVC in 237 patients (61%). Among them, LVEF was the only univariate predictor of outcome. Patients with LVEF ≥45% (n=212) or ≥40% (n=223) had a longer survival than those with LVEF <45% or <40% (p=0.025 and p<0.001, respectively). Conclusions: NDLVC patients, identified by non-ischemic LV scarring and/or fatty replacement and/or hypokinesia and LVEDVi <96 mL/m2 (women) or <105 mL/m2 (men), have a lower risk of death or ventricular arrhythmias than patients with dilated cardiomyopathy. LVEF <45% or <40% further stratified outcome. The definition of NDLVC could incorporate these LVEDVi and LVEF cut-points to identify a population of patients with a homogeneous risk of death or ventricular arrhythmias.