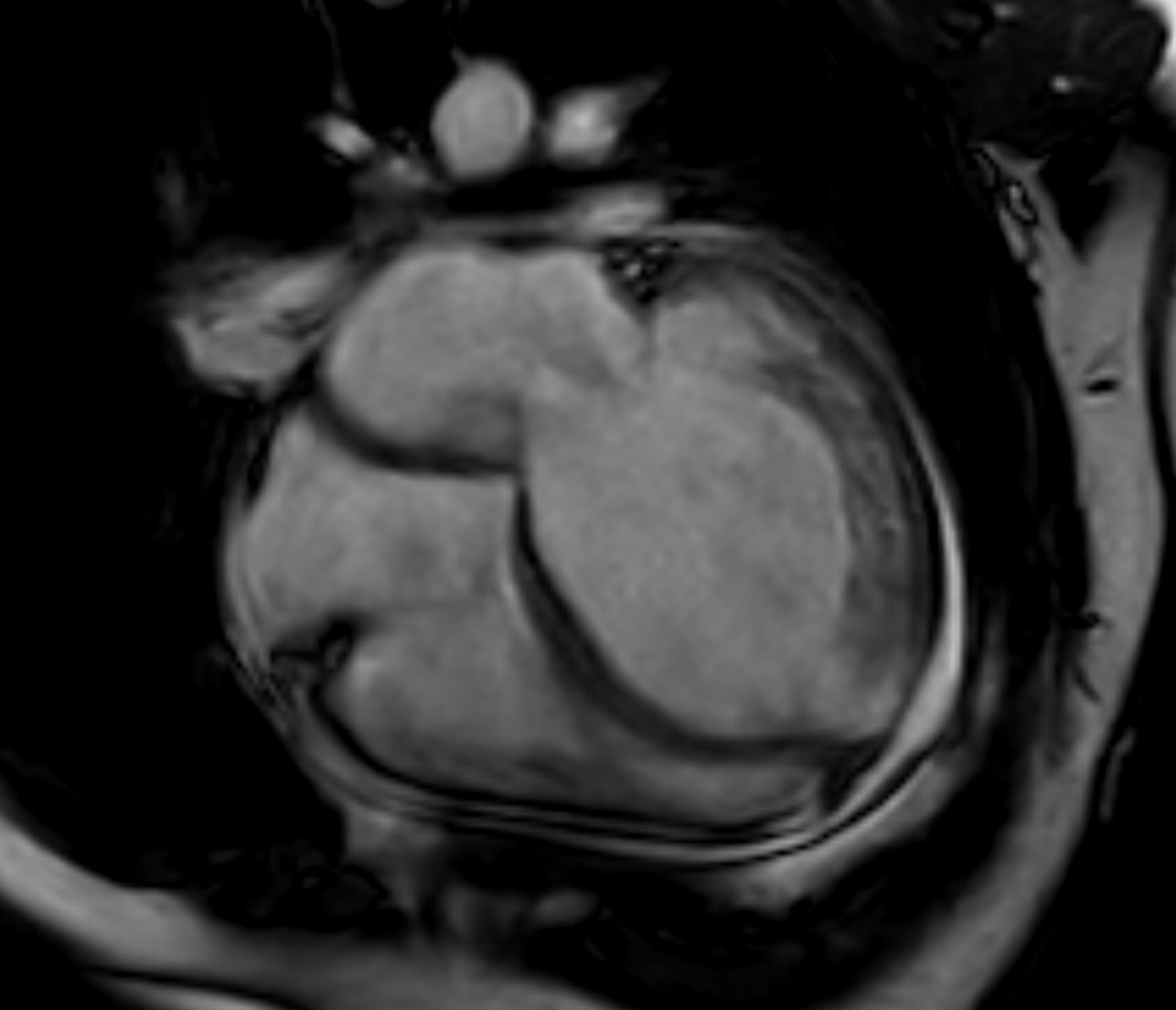
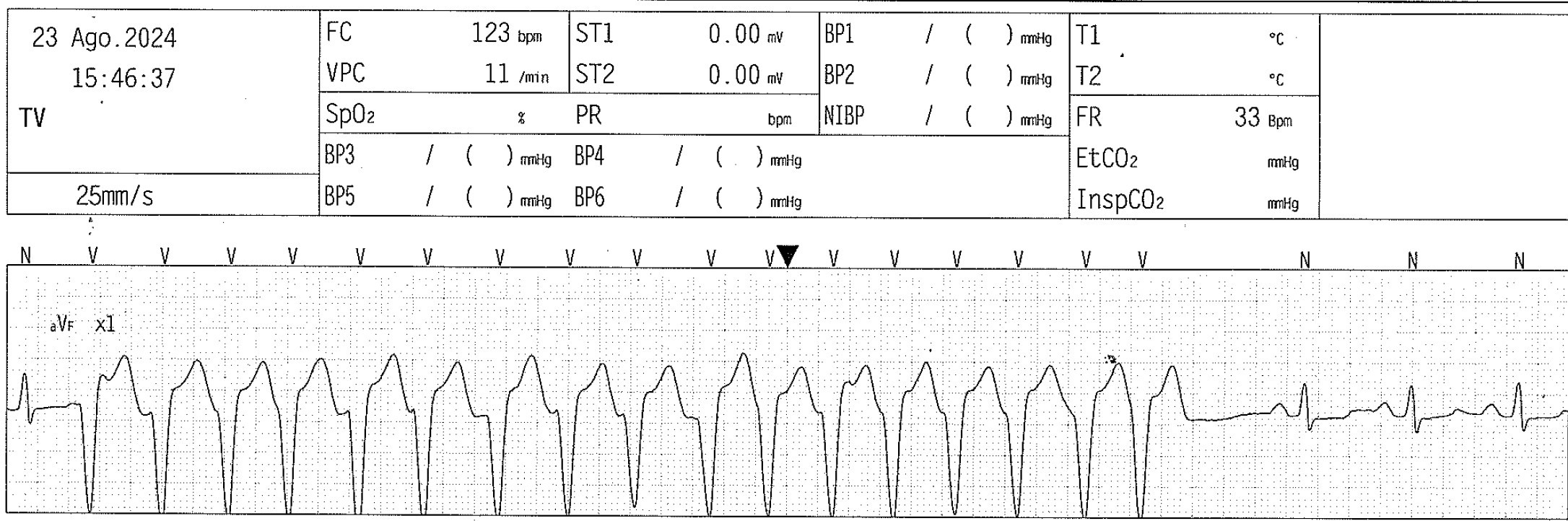
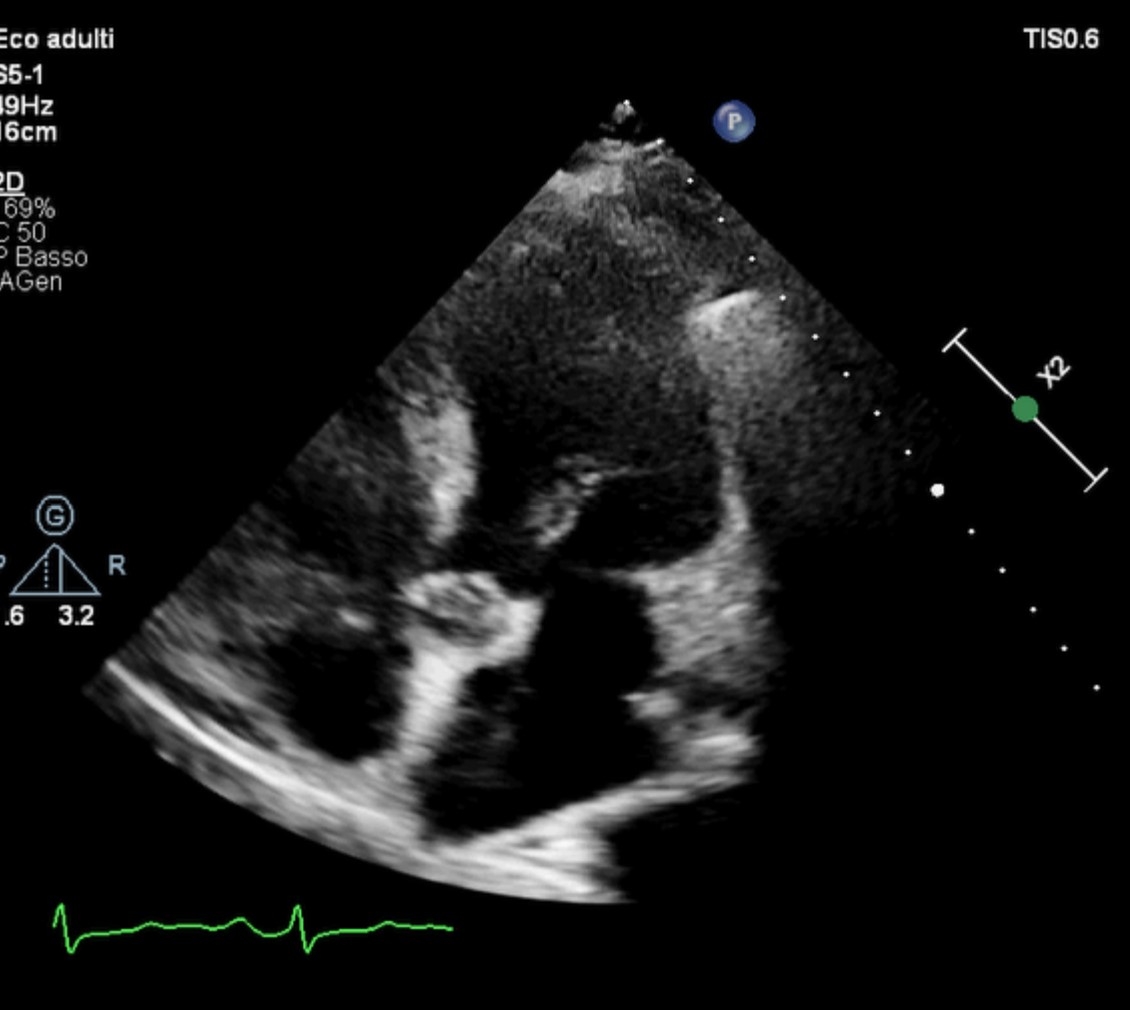
Clozapine is the most effective medication for treatment of refractory schizophrenia, but it is associated with severe cardiac adverse events including myocarditis and cardiomyopathy. Clozapine-induced cardiomyopathy is more chronic than myocarditis with most cases may be due to undetected myocarditis progressing to dilated cardiomyopathy. Some patients experience a rapid decline in cardiac function and these toxicities are diagnosed for the first time at autopsy. We present the case of a 40-years-old male, smoker, with schizophrenia in therapy since 2015 with clozapine. The patient was hospitalized for worsening dyspnea, without chest pain or fever. The ECG showed sinus tachycardia with signs of left ventricular overload. No increase in flogosis index (PCR 0.6 mg/dl), no troponin movement, proBNP level 4800 pg/ml. At chest X-ray a bilateral pleural effusion was present. Echocardiogram showed dilated and spherical left ventricle (end-diastolyc diameter 80 mm), with severe reduction of ejection fraction (20%) and restrictive diastolic pattern, moderate functional mitral regurgitation and moderate tricuspid regurgitation. A therapy with furosemide, sglt-2 inhibitors, beta blocker, spironolactone and sacubitril-valsartan was started, with gradual clinical improvement. Coronary CT showed thin epicardial vessels without relevant coronary stenosis. Cardiac MRI confirm severe ventricular dilatation sx (VTDi 211 ml/mq), ejection fraction 20% (Fig1), reduced right ventricular function (ejection fraction 39%), no areas of edema and especially no areas of late gadolinium enhancement. Episodes of not-sustained ventricular tachycardia were recorded at ECG monitoring (Fig2). In agreement with collegues psychiatrists, we gradually suspended the therapy with clozapine and replaced it with olanzapine. A wearable cardiac defibrillator was positioned for three months. After this period, with optimal medical therapy for heart failure, the patient maintained satisfactory compensation (NYHA I vs NYHA III). The echocardiogram showed important reduction of left ventricle volumes (end-diastolyc diameter 56 mm) (Fig3), significant improvement of systolic function (ejection fraction 43%), mild mitral and tricuspidal regurgitation. The wearable CD does not recorded arrhythmias and was removed. This case highlights how the suspension of clozapine, together with pharmacological therapy for heart failure, can allow a significant regression of serious forms of dilated cardiomyopathy