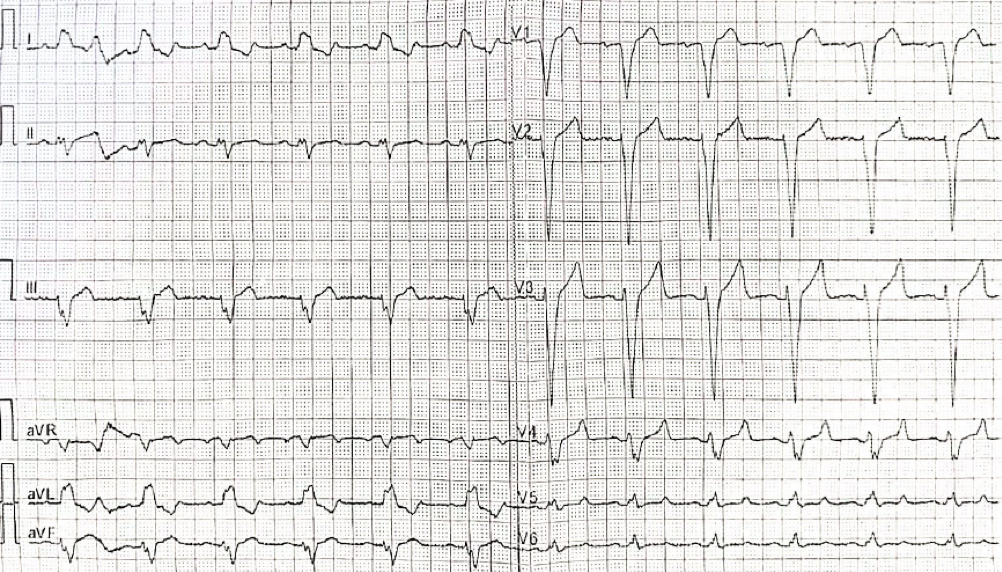
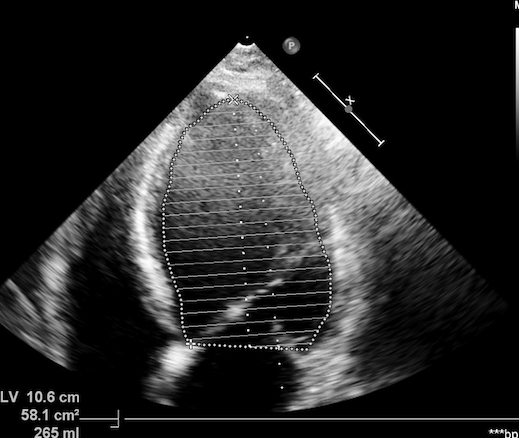
We report the case of a 55-year-old man who presented to the emergency department with fatigability and nocturnal dyspnea. The electrocardiogram showed left bundle branch block. Severe left ventricular dilation (EDV 265 ml) and dysfunction with ejection fraction (EF) 25-30% were found on the echocardiogram. The NT proBNP was 1.497 pg/ml. No coronary artery disease was revealed by the coronary angiography. The cardiac magnetic resonance showed a severely dilated left ventricle with EF 22%, extensive areas of intramyocardial fibrosis with a non-ischemic pattern at the level of the basal segments, anterior, anterolateral and inferolateral medial wall and medial inferior septum of the left ventricle. Frequent ventricular ectopic beats were detected on the electrocardiographic monitoring. Medical therapy with ACE-I, beta-blocker, SGLT2i and MRA was started and after three months the patient underwent CRT-D implantation (QRS 130 msec) for persistent left ventricular dilation with EF 33-35%. In the following months the patient reached good functional capacity with NYHA class I and therapy was optimized with the insertion of sacubitril/valsartan. In subsequent echocardiographic checks, a progressive improvement of EF 45-47% was observed despite the extension of myocardial fibrosis. The outcome of the genetic analysis was positive for a mutation compatible with arrhythmogenic cardiomyopathy: the mutation of the Desmoplakin gene with the substitution of arginine with a stop codon, which, according to the ACMG guidelines, is classified as a pathogenic variant (class 5) Correlation studies demonstrated that, among patients carrying DSP pathogenic/likely pathogenic genetic variants, a wide clinical and instrumental spectrum is present. Recently “Desmoplakin cardiomyopathy” was qualified as a distinct form of cardiomyopathy characterized by frequent left ventricular involvement with extensive fibrosis, high arrhythmic risk, and episodes of acute myocardial injury. Classical variables routinely used for risk estimation in DCM and ACM populations appear inadequate and fail to predict the arrhythmic risk in DSP cardiomyopathy. In our case, the left bundle branch block and severe left ventricular dysfunction made clear the necessity of CRT-D before genetic test results become available. Dedicated tools to predict risk and to guide ICD implantation remain an unmet need in the management of DSP carriers.