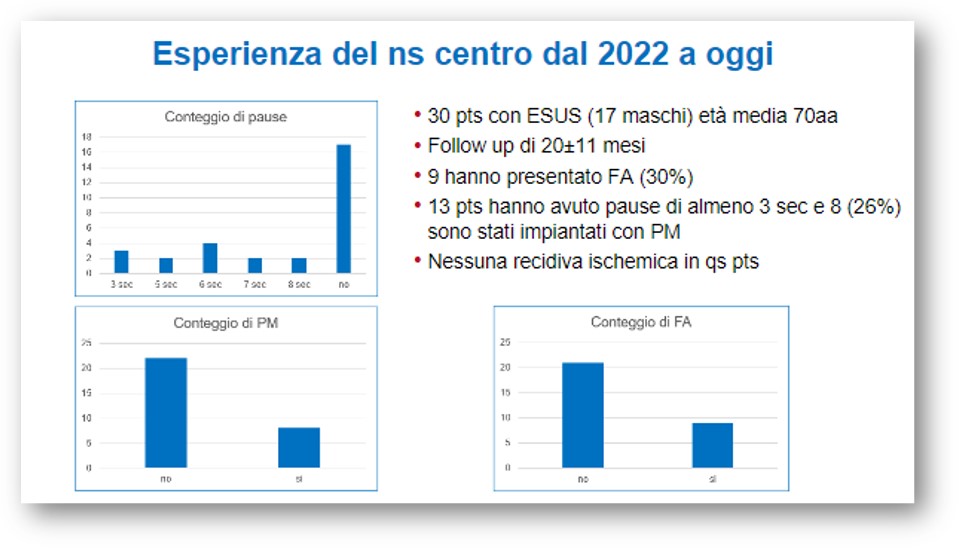
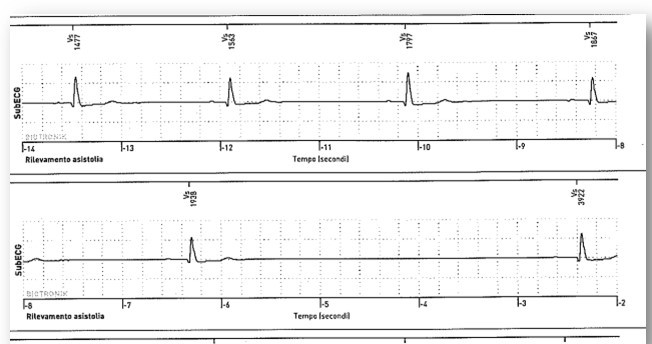
Implantable loop recorder (ILR) can be used to detect subclinical atrial fibrillation (AF) in patients with embolic stroke of undetermined origin (ESUS). In literature the incidence of AF is about 18% with a risk of recurrence of stroke in antiplatelet therapy of 4.5%. ESUS is a severely disabling stroke with high mortality rate.To improve the search of causes of ESUS a good collaboration between Cardiologist and Neurologist is essential. Is not yet defined the optimal ECG monitoring lenght in ESUS patients, and has not been established the use of anticoagulant versus antiplatelet therapy in patients without detected AF. In our Hospital we evaluated and implanted loop recorder in patients with ESUS from January 2022 to March 2024, for detection of subclinical AF or other arrhythmias and followed them with remote monitoring. Before implantation, all patients were submitted to standard protocols for the identification of the causes of stroke with computed tomography or brain magnetic resonance; there were no stenosis > 50% in extra and intracranial vessels, absence of major cardioembolic sources (AF or flutter, ventricular thrombosis, severe left ventricular dysfunction with ejection fraction < 30%, infectious endocarditis), arteritis, vascular dissection, vasospasm. We enrolled a group of 30 patients, 17 men and 13 women, mean age 70 +- 11 years, with 26 strokes and 4 transient ischaemic attack; all these patients were implanted with ILR. The average follow-up was 20 +-11 months. Atrial tachyarrythmies were detected in 9 patients (30%). Episodes of sinus arrest were reported in 13 patients (43%) and 8 (26%) had pauses more then 6 seconds requiring two-chamber pacemaker implantation, 3 of these patients had also AF (10%). In 3 patients pauses were short and remained in follow-up. In 6 patients (20%) oral anticoagulant therapy was begun, due to the finding of episodes of atrial fibrillation of long duration or high frequency. Monitoring patients with ILR is confirmed to be useful in ESUS. Our experience with the limit of the numerosity and the follow-up not very long, shows data in line with literature. The incidence of AF is comparable, but the incidence of bradyarrhythmias, which required pacemaker implantation mainly sinus arrest, is higher. These data are interesting and useful for the therapeutic path of patient, to reduce the risk of recurrence of stroke that appears a problem of great importance personal, economic and social.