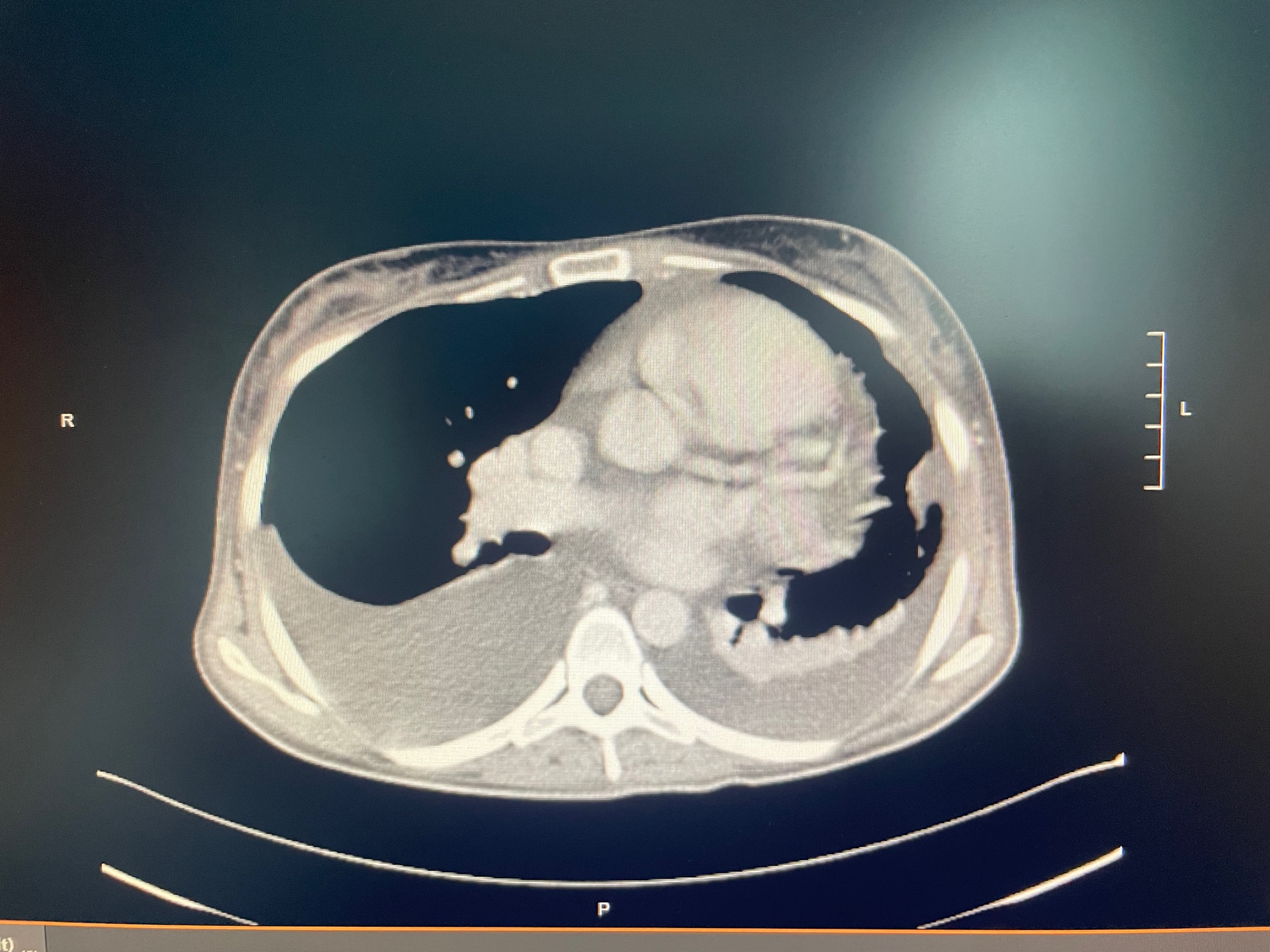
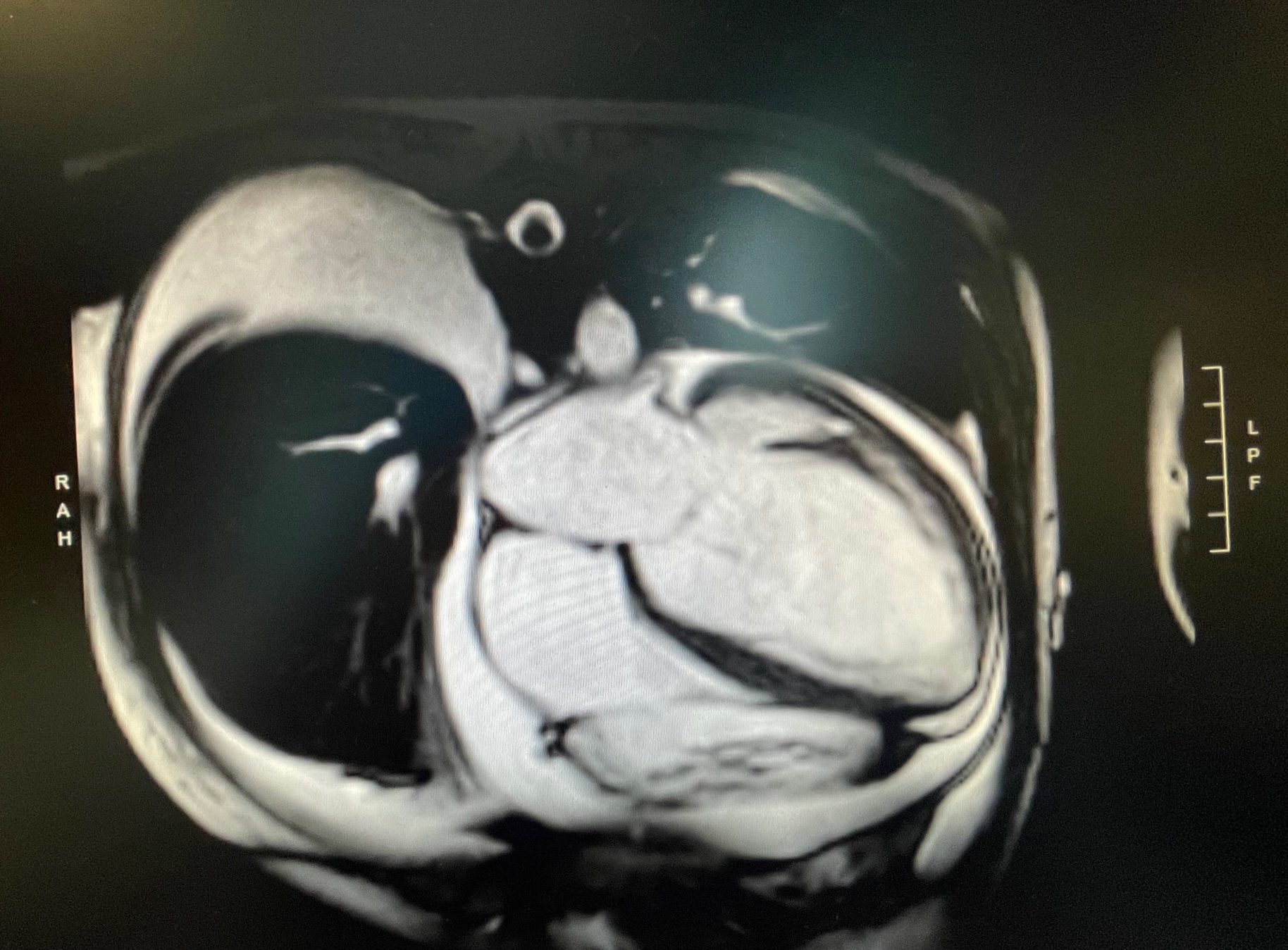
Anemia is a common comorbidity in patients with heart failure (HF). Less frequently anemia is the primary cause of HF and acute HF as the first manifestation of low hemoglobin levels is rarely described. A 26 year old women, affected by mild eating disorder (BMI 18.4 Kg/mq), presented to the ED because of fatigue and signs of congestion, which begun a few weeks prior. No bleeding had ever occurred. Laboratory tests showed severe anemia (Hb 2.7 g/dL), severe increase in proBNP (8668 pg/mL) and a severe iron deficiency. TnTHS was normal. The echocardiogram showed severe left ventricular dilation (EDV 162 ml), with moderate dysfunction (EF 40%) and a mild right ventricle dysfunction. Cardiac MRI confirmed echocardiographic findings, excluding edema or fibrosis. Blood transfusions, iron supplementation and intravenous furosemide allowed a rapid improvement of the picture and a normalization of hemoglobin (Hb 12 g/dL at discharge). Heart failure therapy with ACE-inhibitor, betablocker and MRA was implemented during the hospitalization. A close follow-up was carried out at the HF clinic after the discharge. Six weeks later, the clinical picture had improved in spite of an unchanged echocardiogram. Dapaglifozin was therefore prescribed. In the following months, the titration of HF therapy was slowed by hypotension and ARNI was started only 4 months later. It is worth emphasizing that, subsequently, echocardiographic parameters progressively improved, with a complete normalization of left ventricular volume, an increase in EF (52%) and a complete normalization of right ventricular function after 10 months. This clinical case provides some considerations: HF due to removable causes has not always a benign course. The improvement in cardiac function was slow and not fully complete in our case, in spite of the young age We observed an improvement of EF just after the introduction of ARNI Even after the complete normalization of the hemoglobin and the implementation of the four pillars, cardiac function remained at the lower limit of the normal range. This could be probably due to the time elapsed between the onset of the causal condition and the onset of medical therapy. Plausibly the decrease in hemoglobin was very slow, since the patient sought medical attention when it had already dropped to 2.7 gr/dL We believe that HF therapy should never be suspended in this patient and that her management would be extremely challenging if she desired a pregnancy.