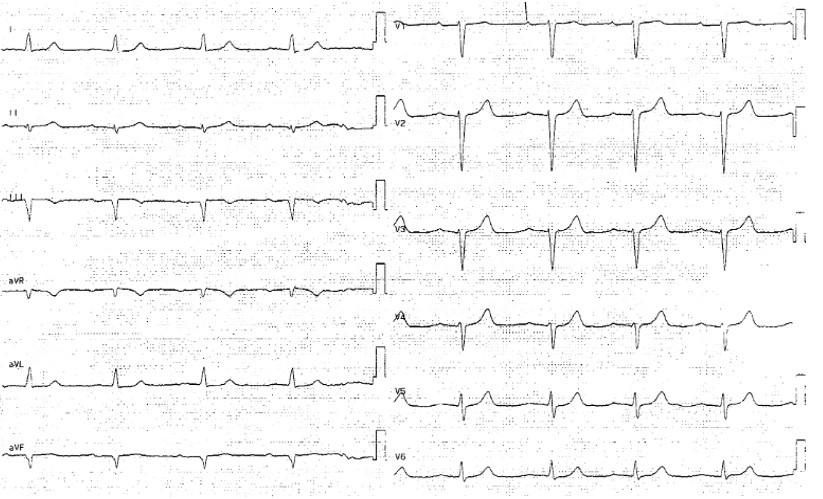
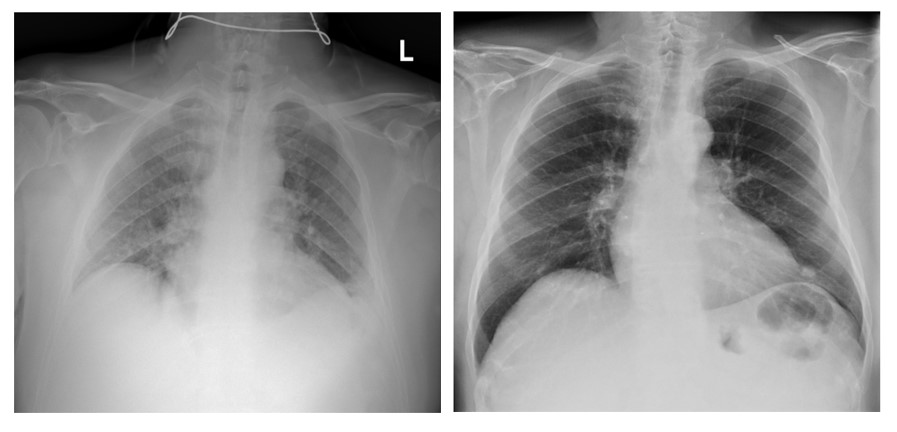
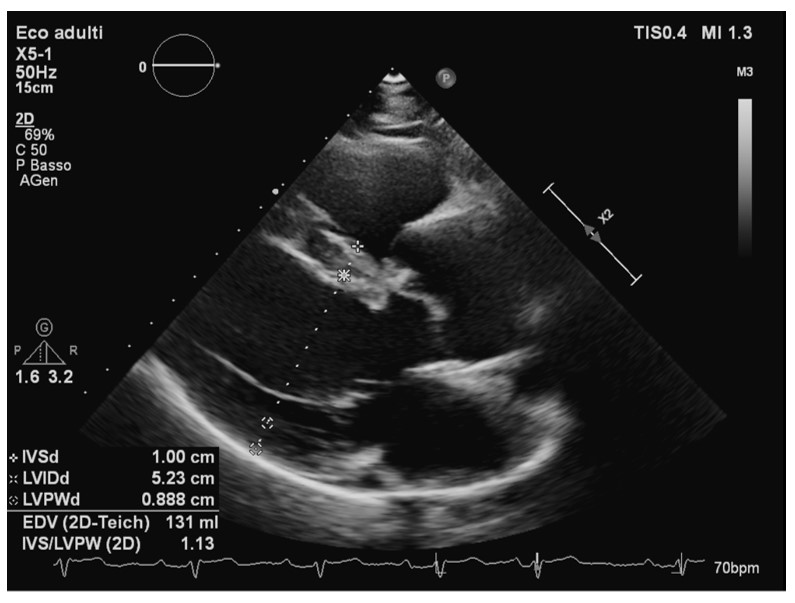
Flecainide is an effective antiarrhythmic agent for atrial fibrillation (AF) cardioversion, particularly in patients without significant structural heart disease. However, it may cause hemodynamic compromise in patients with left ventricular dysfunction. A 71-year-old man presented to the emergency department with worsening dyspnea and asthenia two days after undergoing electrical cardioversion for AF, during which flecainide therapy was initiated. The patient had previously undergone electrical cardioversion with amiodarone, which resulted in early recurrence. Additionally, coronary angiography performed a few months earlier had revealed no significant coronary artery disease, and a prior echocardiogram had shown normal findings. At presentation, echocardiography showed moderate-to-severe biventricular dysfunction, mild mitral insufficiency, and mild-to-moderate tricuspid insufficiency with reduced caval collapsibility. The ECG revealed sinus bradycardia at 52 bpm, first-degree atrioventricular block, left axis deviation, poor R-wave progression in the precordial leads, normal repolarization, and a QTc of 484 ms. Arterial blood gas analysis indicated hyperventilation and reduction of bicarbonates (pH 7.45, pO2 97 mmHg, pCO2 27 mmHg, HCO3- 18.8 mmol/L, Lac 1.3 mmol/L). A chest X-ray showed hilar congestion with a small left pleural effusion. Laboratory tests revealed acute kidney injury stage 2 and worsening liver function parameters (creatinine 2.02 mg/dL, urea 110 mg/dL, AST 81 U/L, ALT 171 U/L) compared to values from two days earlier (creatinine 0.97 mg/dL, urea 50 mg/dL, AST 33 U/L, ALT 58.7 U/L). On admission to the ward, diuretic therapy with low-dose furosemide was initiated, resulting in rapid symptomatic relief. Flecainide therapy was discontinued. Liver and kidney function showed marked improvement within two days. A follow-up echocardiogram revealed a significantly improved cardiac function profile, with normal biplane ejection fraction (FE 58%), mild mitral regurgitation, normal right ventricular dimensions and systolic function (TAPSE 21 mm), and mild tricuspid regurgitation. This case highlights acute biventricular dysfunction likely induced by flecainide, with complete recovery following drug discontinuation. It underscores the importance of vigilance regarding this potential adverse effect of flecainide.