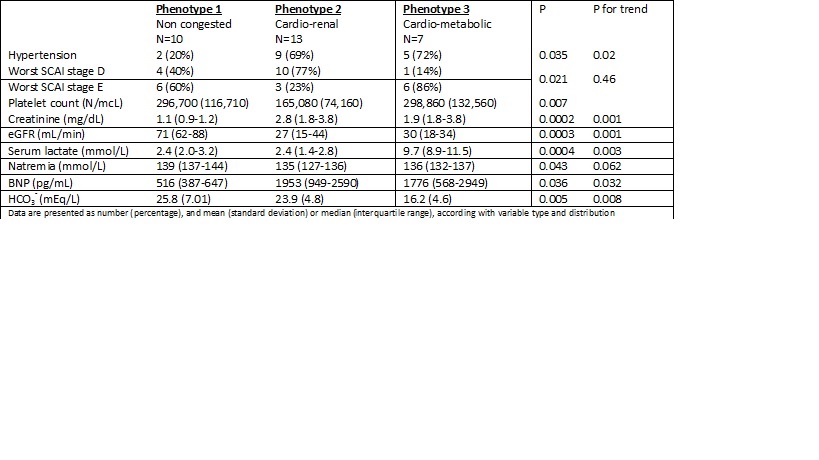
Backgroud: Cardiogenic shock (CS) is a clinical syndrome defined by tissue hypoperfusion due to low cardiac output. It is characterized by extreme heterogeneity in etiologies, severity, and underlying pathophysiology. Phenotypes in CS population identified using unsupervised machine learning clustering methods have been proposed, potentially facilitating understanding the underlying pathophysiology, prognosis, and appropriate treatment. The present study aims to characterize the contemporary real-world population of patients admitted to our center for CS and their prognosis according to this cluster classification. Methods: We conducted a retrospective observational analysis of all consecutive patients admitted to our center for CS from January 2023 to July 2024. Enrolled patients were classified into three phenotypes (I – non congested, II – cardio-renal, III – cardio-metabolic) according to the Cardiogenic Shock Working Group – Society of Cardiovascular Angiography and Intervention (CSWG-SCAI) shock phenotype calculator. Demographic, clinical and outcome data were than compared to identify any differences across phenotypes. Results: A total of 30 patients were enrolled in the study, with a mean age of 70±14 years, 24 (80%) were male, 9 (30%) had diabetes, and in 7 (23%) the main reason for CS was an acute myocardial infarction. According to CSWG-SCAI calculator, 10 patients were classified in phenotype I (33,3%), 13 in phenotype II (43,4%), and 7 in phenotype III (23,3%). Variables that differed significantly between phenotypes are presented in Table 1. Hypertension was more prevalent in phenotypes II and III (respectively 69% and 72% vs 20%; p=0.035). Worst SCAI stage D was observed mostly in phenotype II (76%) and SCAI stage E in phenotype III (86%; p=0.02). We observed higher levels of BNP in phenotypes II and III. Phenotype II was characterized by worse renal function on admission and phenotype III by a higher serum lactate concentration with reduced bicarbonates. Mortality was higher in phenotype III (57.1%), and similar in phenotypes I and II (30 and 30.8% respectively), although not reaching statistical significance (p=0.44). Conclusions: In our real-word, contemporary cohort of patients admitted for CS, different phenotypes as defined by CGWG-SCAI calculator, are characterized by different clinical profile and possible different prognosis. Phenotyping cardiogenic shock could help to improve clinical management and prognosis of patients with CS