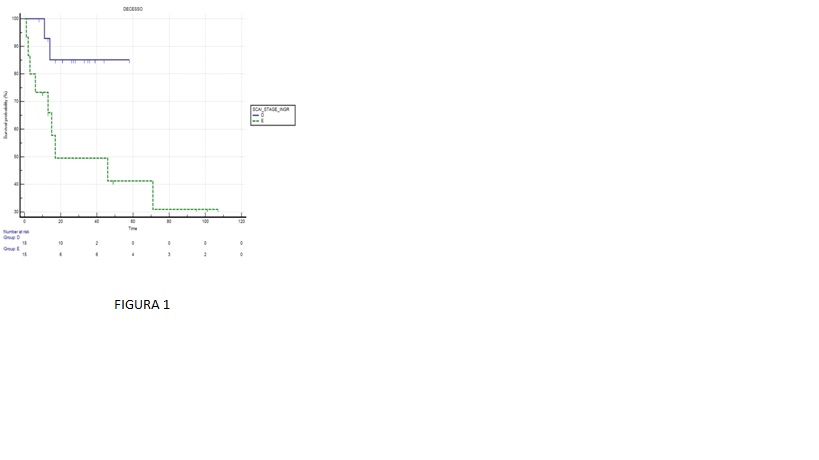
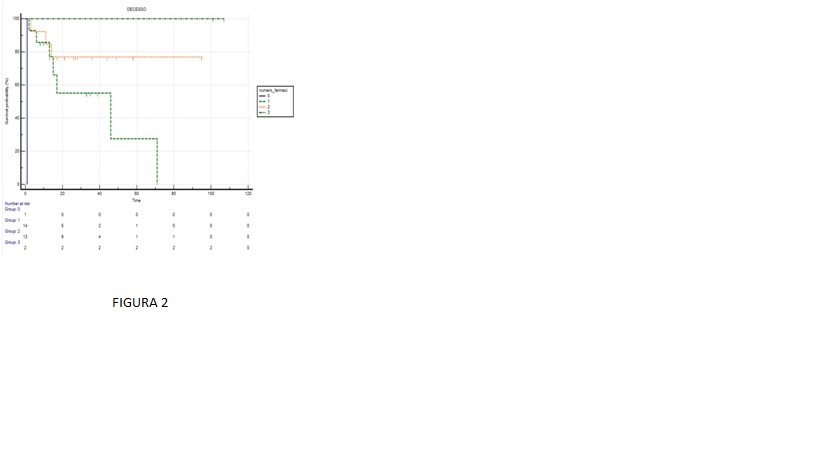
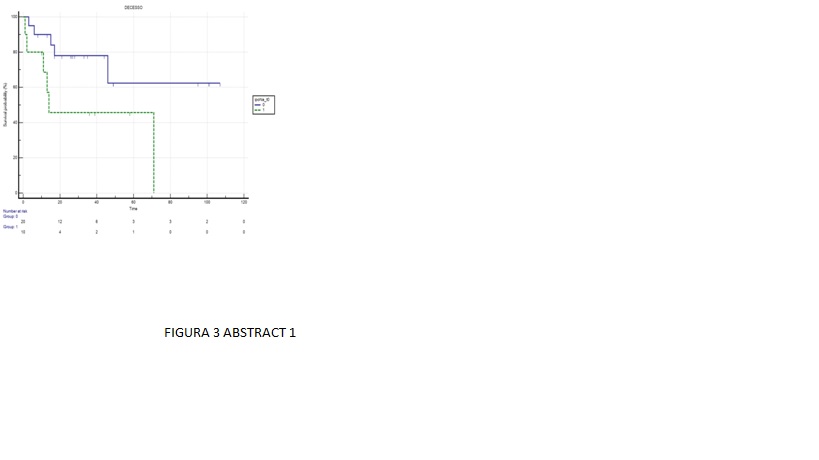
Background: Cardiogenic shock (CS) is a life-threatening syndrome characterized by a low cardiac output, followed by tissue hypoperfusion and increased lactate levels, which frequently leads to multi-organ failure and death. Despite the improvements in clinical management and therapeutic approach, in-hospital mortality remains high. The aim of the present study was to analyze the incidence and predictors of in-hospital mortality in patients admitted for CS in our cardiac intensive care unit (CICU). Methods: We conducted a retrospective observational analysis of all consecutive patients admitted in our CICU for CS from January 2023 to July 2024. Demographic, clinical and outcome data were retrieved from medical records. The primary outcome was the incidence of in-hospital all-cause mortality. Its predictors were analyzed using univariate logistic regressions. Moreover, a time-to-event analysis was performed according to Kaplan-Meier method. Results: During the enrolling period, 30 patients met the inclusion criteria. The mean age was 70±14 years, 24 (80%) were male, 16 (53%) had hypertension, 9 (30%) diabetes, and in 7 (23%) the main reason for CS was an acute myocardial infarction. The median hospital stay was 23.5 (IQR 13-44) days. The SCAI stage at presentation was B in 4 patients (13.3%), C in 4 (13.3%), D in 14 (46.7%) and E in 8 (26.7%). A pharmacological inotropic/vasopressor support was started in 29 patients (97%) and a mechanical circulatory support was needed in 7 cases (23%). Eleven patients (37%) required invasive ventilation. The overall in-hospital mortality was 36.7% (95% CI 19.9-56.1%). The worst SCAI stage during hospitalization was associated with higher in-hospital mortality (SCAI D vs E, OR 0.103, 95% CI 0.017-0.628, P=0.0134, P log rank=0.0366 – Figure 1). Furthermore, the use of a greater number of inotropic/vasopressor drugs (OR 0.223, 95% CI 0.053-0.948, P=0.0421, P log rank < 0.0001 – Figure 2), and a higher level of natremia on admission (OR 0.836, 95% CI 0.746-0.998, P=0.0473, P log rank for hyponatremia=0.0413 – Figure 3), were associated with lower mortality. Conclusions: In our real-word, contemporary, CICU cohort of patients admitted for CS, the in-hospital mortality was significantly high and overall consistent with previous data available in the literature. The main features that influenced it were the worst SCAI stage during hospitalization, hyponatremia on admission, and the number of inotropes/vasopressors used.