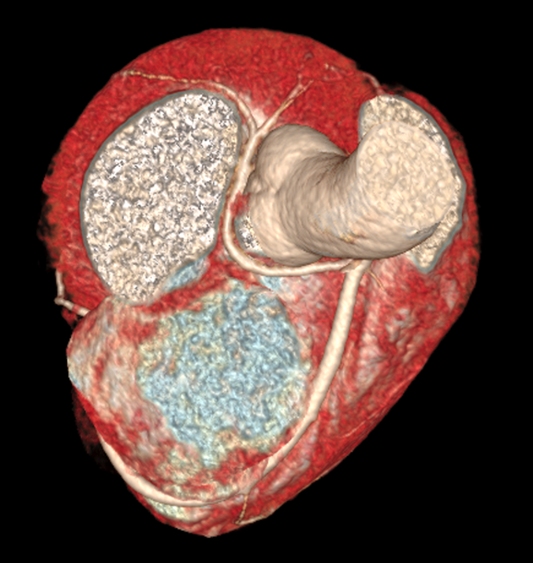
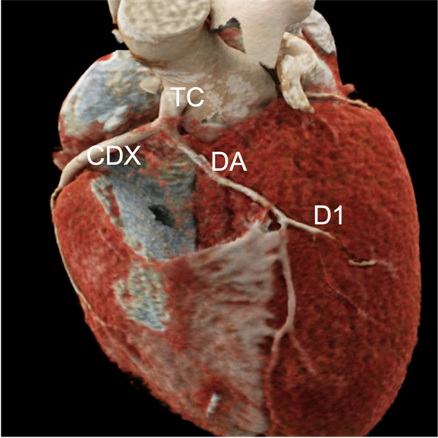
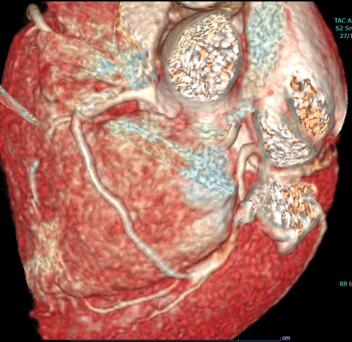
Anomalous coronary arteries (ACA) represent an anomalous location of the coronary ostium and/or vascular course. Although most individuals with ACA are asymptomatic, some ACA variants are leading to symptoms and adverse cardiac events. In particular, isolated single coronary artery (iSCA) arising from the right sinus of Valsalva, is a rare congenital coronary anomaly and represents approximately 2% to 4% of ACA. Lipton et al were the first to classify iSCA anomalies. Case 1: 26 years old boy, evaluated for palpitations at age of 11. No history of chest pain or syncope. Soccer player. Due to the suspect of coronary anomaly by transthoracic echo with evidence of single coronary artery originating from right sinus of Valsalva, retroaortic course of left circumflex artery and anterior course of left anterior descending (LAD) toward the right ventricular outflow tract, we performed a cCTA that confirmed a single coronary artery originating from the right sinus; LAD with subpulmonic course with trans-septal segment, before emerging to the epicardial surface of the left ventricle (Type RIII LAD-S, LCX-P, Lipton Classification). Resting and during effort ECG showed normal sinus rhythm without ischemic anomalies, Holter monitoring no evidence of arrhythmias. No LGE at MRI was demonstrated and stress MRI was negative for sign or symptoms of ischemia. Case 2: 15 years old boy, evaluated for cardiac murmur at age of 10 (5 yr of follow up). TTE suspected the coronary anomaly with evidence in short axis view of two vessels of equal size, coming from the RSV, one direct toward the right atrioventricular groove (right coronary artery, RCA) and LMCA with anterior course. No vessel originating from left sinus of Valsalva was detected. Resting and during effort ECG showed normal sinus rhythm without ischemic anomalies, Holter monitoring was unremarkable for arrhythmias. cCTA highlighted the single coronary artery arising from the RSV; left coronary artery courses anterior to the pulmonary artery, surrounding the RV outflow tract (prepulmonic course) giving raise to LAD and LCX, (Type RII-A, Lipton Classification). No medical treatment ongoing. Both patients were scheduled for cardiac surgeon consultation and they are, at the moment, on clinical follow up. The first patient is free for palpitations, with beta blockers therapy. Recommendations is to avoiding heavy exercise. During the follow up period there were no mayor events attributable to the iSCA.