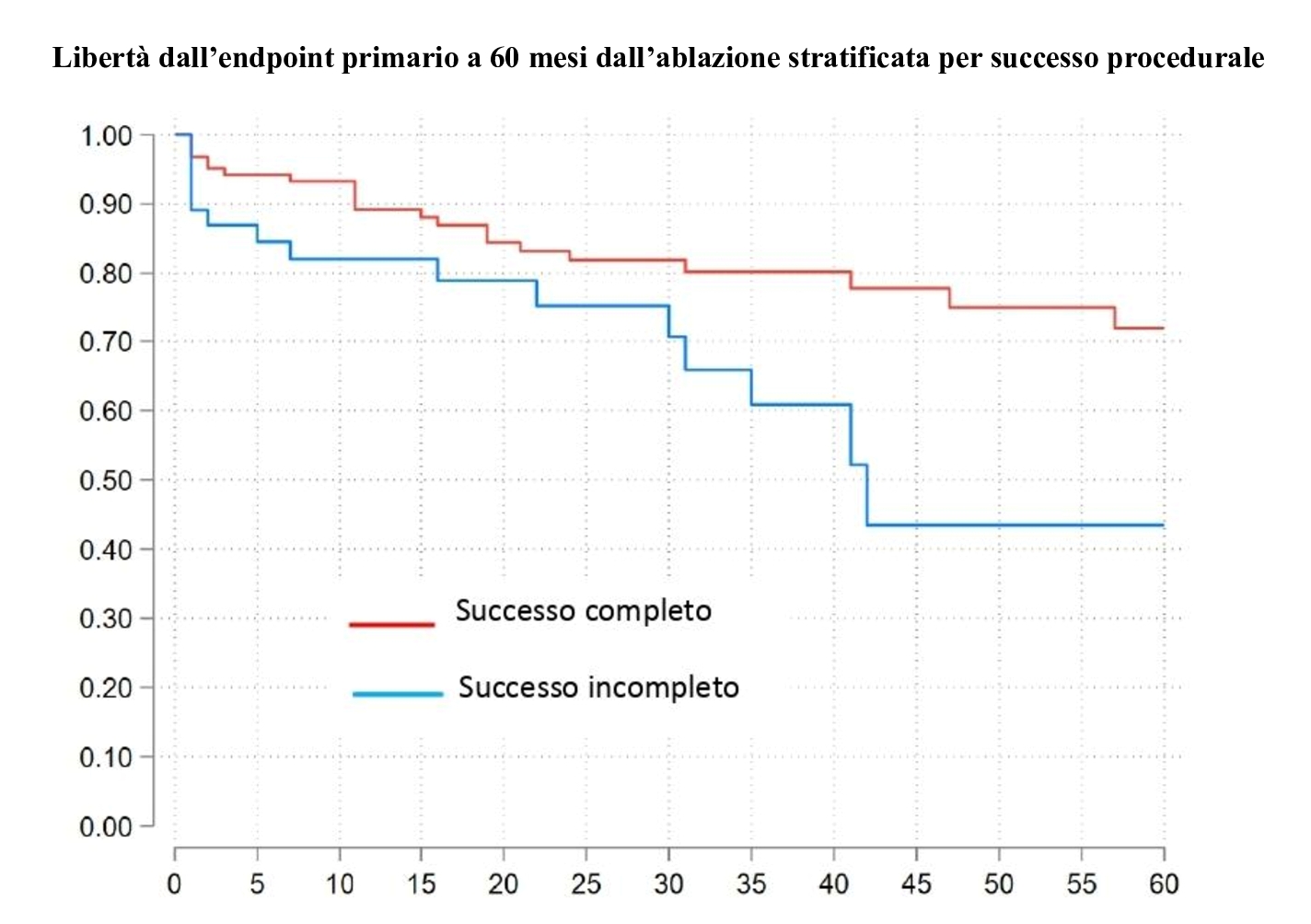
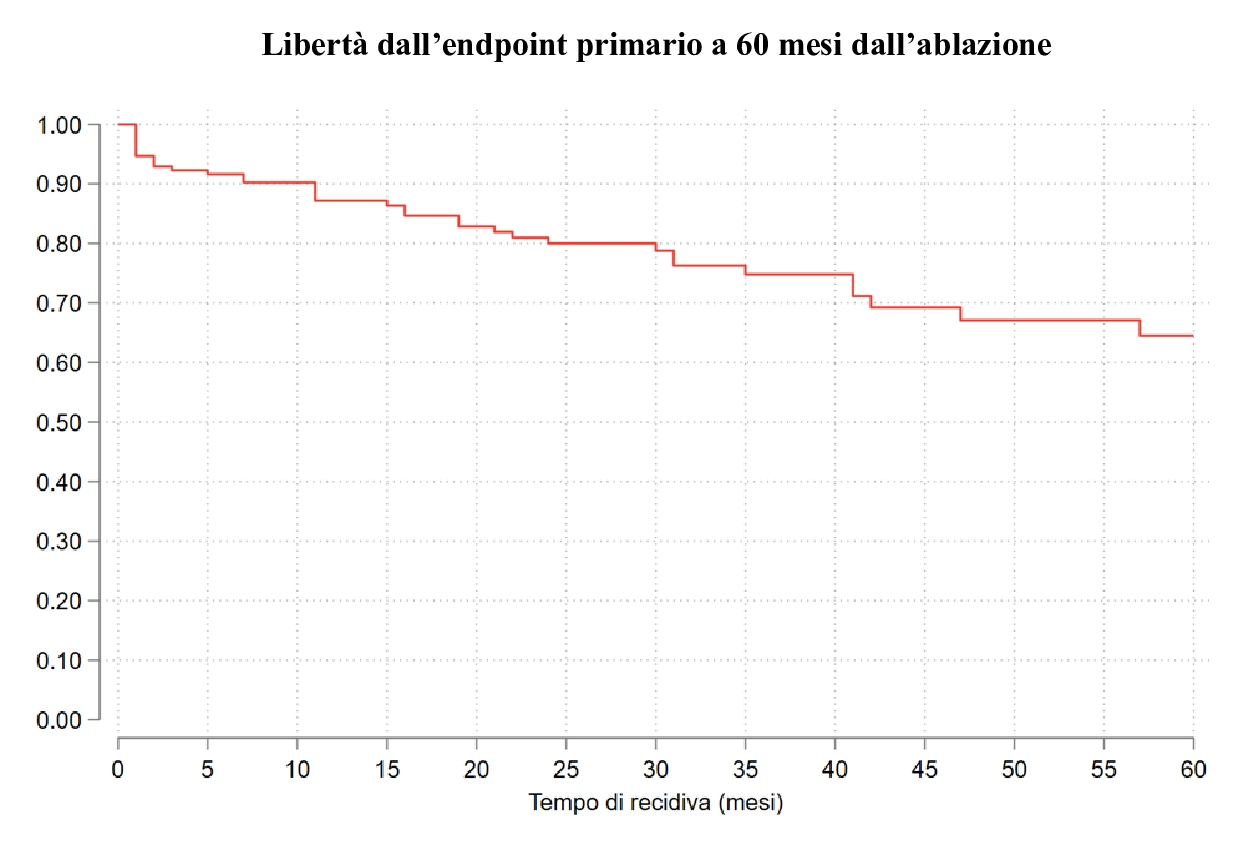
BACKGROUND In patients with monomorphic ventricular tachycardia (VT), structural heart disease (SHD), and preserved or mildly reduced left ventricular ejection fraction (LVEF), catheter ablation (CA) can be considered an alternative or a complementary therapy to an implantable cardioverter defibrillator (ICD). To date, limited data are available on how patients with VT and mildly reduced LVEF are managed in clinical practice and on the effectiveness of CA in this population. AIM To evaluate clinical outcomes of patients with VT, SHD and LVEF ≥ 40% undergoing CA, with or without ICD implantation, enrolled in an international multicenter registry. METHODS A total of 205 patients (median age 69 years, median LVEF 55%, 94% NYHA ≤ 2) underwent CA for hemodynamically well-tolerated VT. 56% had ischemic cardiomyopathy, 12% dilated cardiomyopathy, 11% arrhythmogenic right ventricular cardiomyopathy. 68% of patients (141/205) received an ICD following the CA procedure. Primary endpoint was a composite of VT recurrence, sudden cardiac death (SCD), or ICD intervention for VT. Secondary endpoint was VT recurrence rates stratified by the procedural success of ablation (complete success, incomplete success or failure). RESULTS Complete success was achieved in 72%, incomplete success in 23%, failure in 5% of patients. Complications were observed in 6% of patients (cardiac tamponade 2%, advanced atrioventricular block 2%). At a median follow up of 60 months primary endpoint occurred in 24% of patients. Freedom from arrhythmic recurrence at 24 months was 80%. Freedom from arrhythmic recurrence was significantly higher in patients with complete procedural success vs. those with incomplete success (72% vs. 43%; p=0.01). No cases of SCD or ICD intervention on ventricular fibrillation were reported. Overall survival at 60 months was 80% in the ICD group and 70% in the non-ICD group (p=0.22). CONCLUSIONS Catheter ablation of sustained monomorphic VT is highly effective in patients with SHD and preserved or mildly reduced EF. Nonetheless, the majority of these patients still receive an ICD, as reflected in our real-world clinical data.