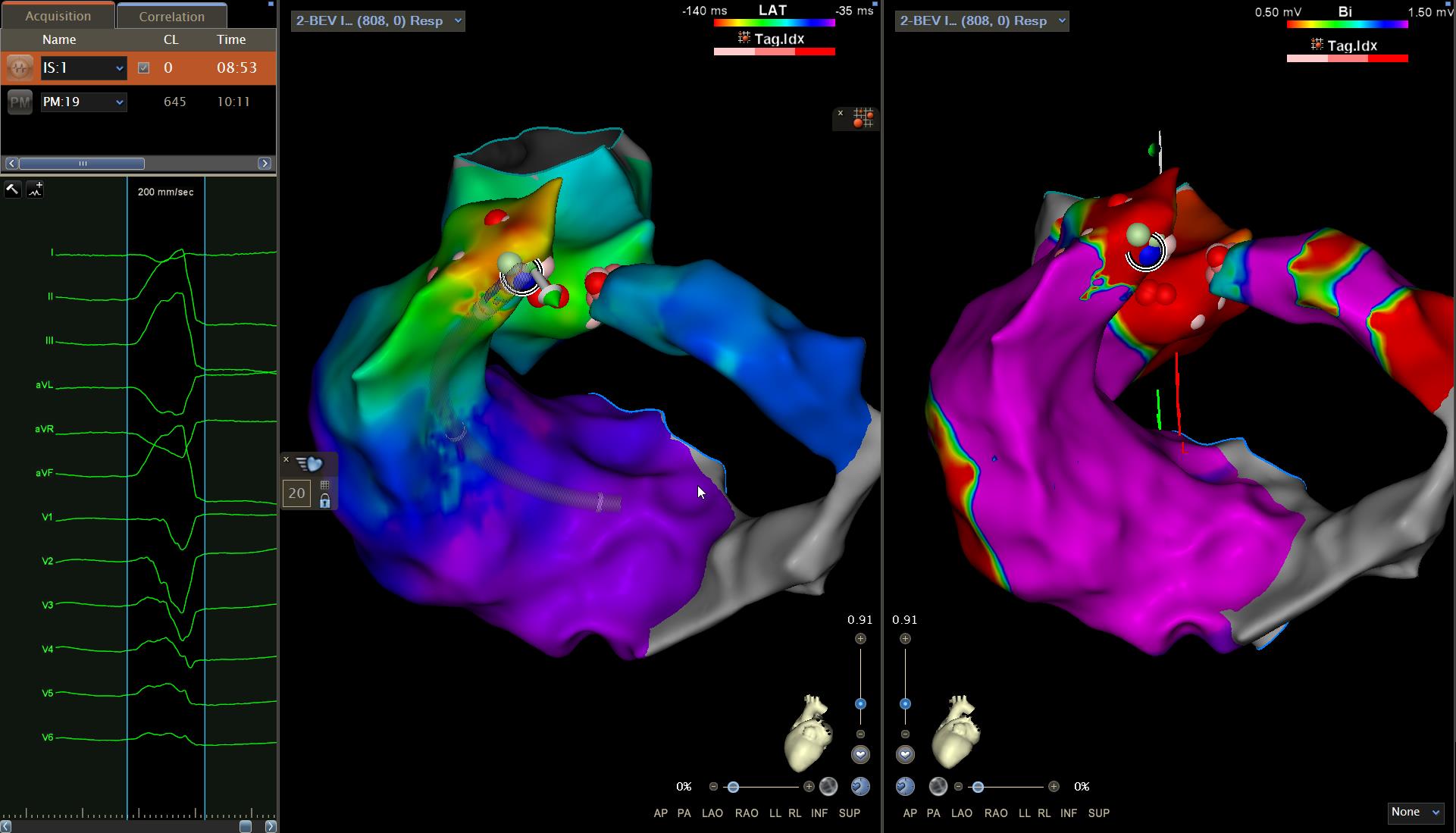
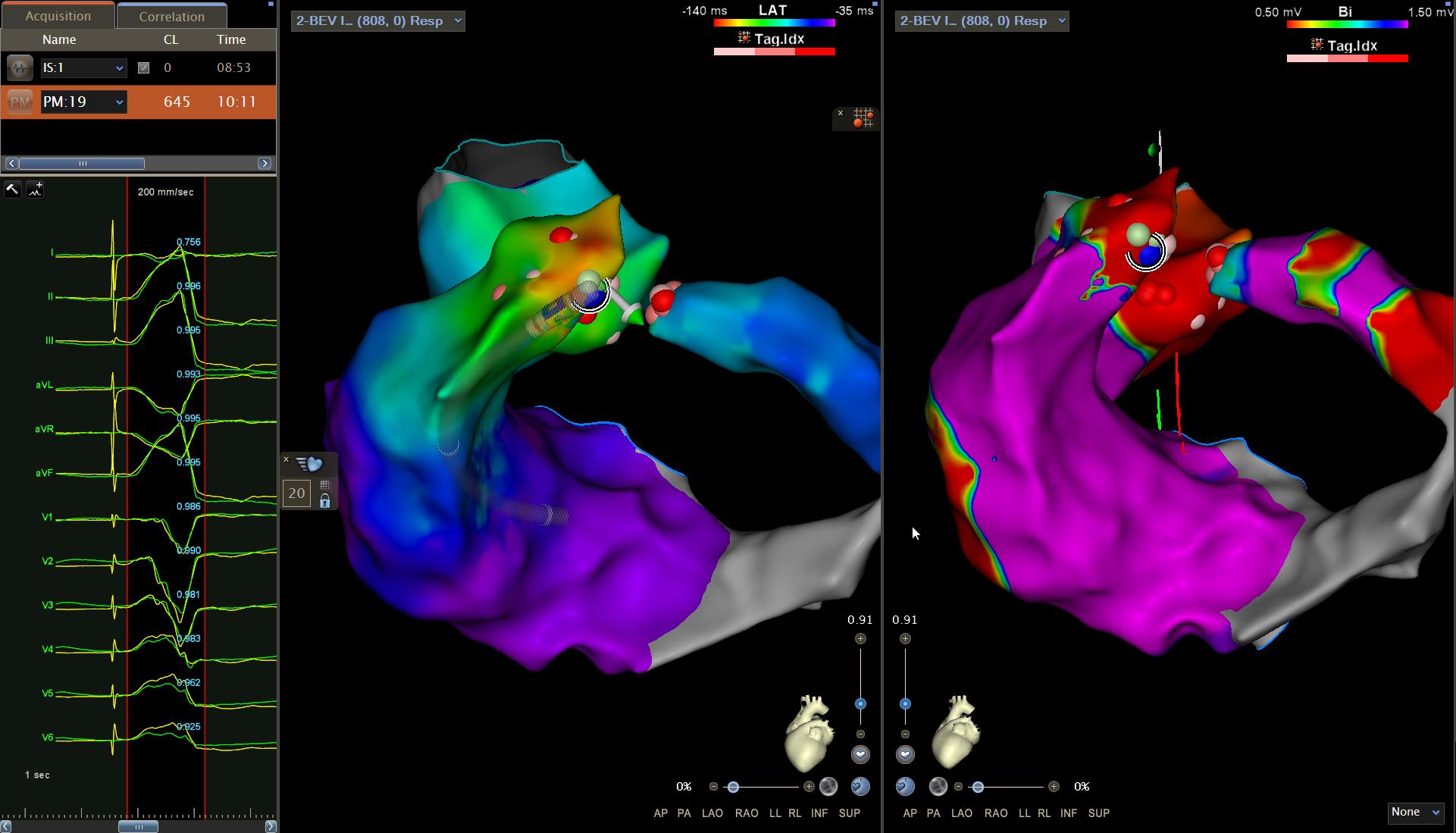
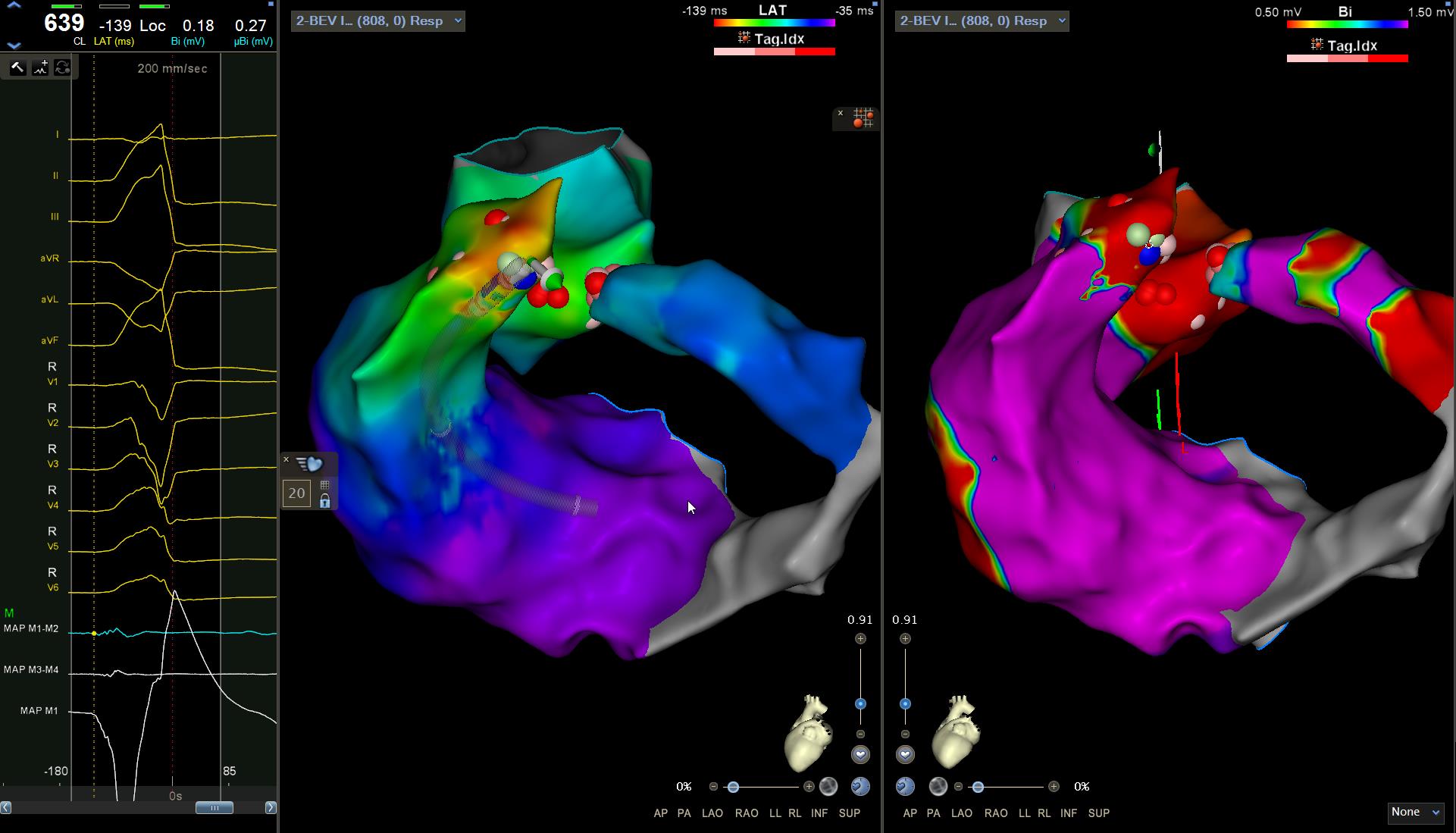
The left ventricular summit (LVS) is a triangular area located in the most superior portion of the left epicardial ventricular region. The approach to the LVS can be performed through the surrounding structures as there is rich coronary arterial and venous vasculature within the confines of the LVS. The ablation of ventricular arrhythmias originating from the LVS is performed by alcoholic ablation of cardiac tissue drained from peripheral branches of the coronary sinus by selectively cannulating the latter. However, this approach cannot often be used due to the technical difficulties due to anatomical variability of the peripheral coronary venous system. This case report shows how to ablate ventricular arrhythmias originating from LVS with an endo-epicardial approach. 74-year-old man suffering from chronic ischemic heart disease previously subjected to PTCA and CABG (left IMA on LAD and right IMA on AML, 2016). Hospitalized at our department for very frequent monomorphic and repetitive premature ventriicular contractions (PVCs) for non-sustained ventricular tachycardia (NSVT). Coronary angiography documented patent bypasses and absence of critical coronary lesions. The echocardiogram documented moderate left ventricular pump dysfunction with alterations in segmental kinetics and mild right ventricular pump dysfunction. Antiarrhythmic therapy with beta-blocker was ineffective for persistence of PVCs and NSVT. Ablation of the ventricular arrhythmias was therefore performed. The electrocatheter was inserted into the outflow tract of the right ventricle, identifying areas of maximum precocity at the septal level (pace-mapping with morphology corresponding to 96% of clinical PVCs). Radiofrequency were applied in this area with a clear reduction in the arrhythmia burden. The arrhythmia in the coronary sinus was mapped in the mirror image of the previously ablated area, identifying the area with good precocity. Radiofrequency was applied on this site with a further reduction in the arrhythmic burden without, however, achieving complete extinction of the PVCs. Further ablation was performed in the outflow tract of the left ventricle in the mirror image of the previously ablated areas, obtaining complete extinction of the arrhythmias. No arrhythmic relapses at subsequent monitoring. In this case the endo-epicardial approach for the ablation of the PVCs originating the LVS was effective, as already demonstrated by our series of ablation of these arrhythmias.