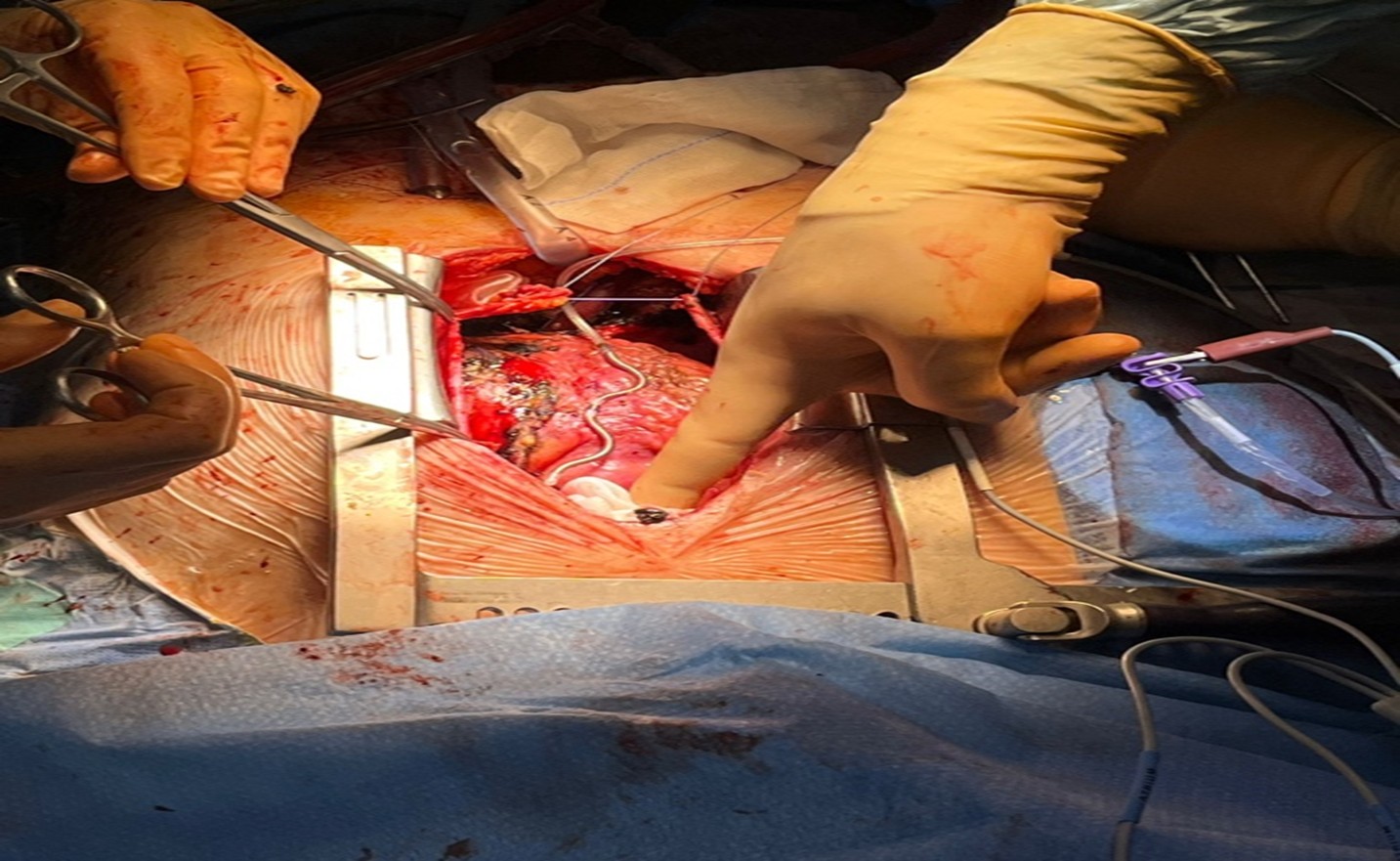
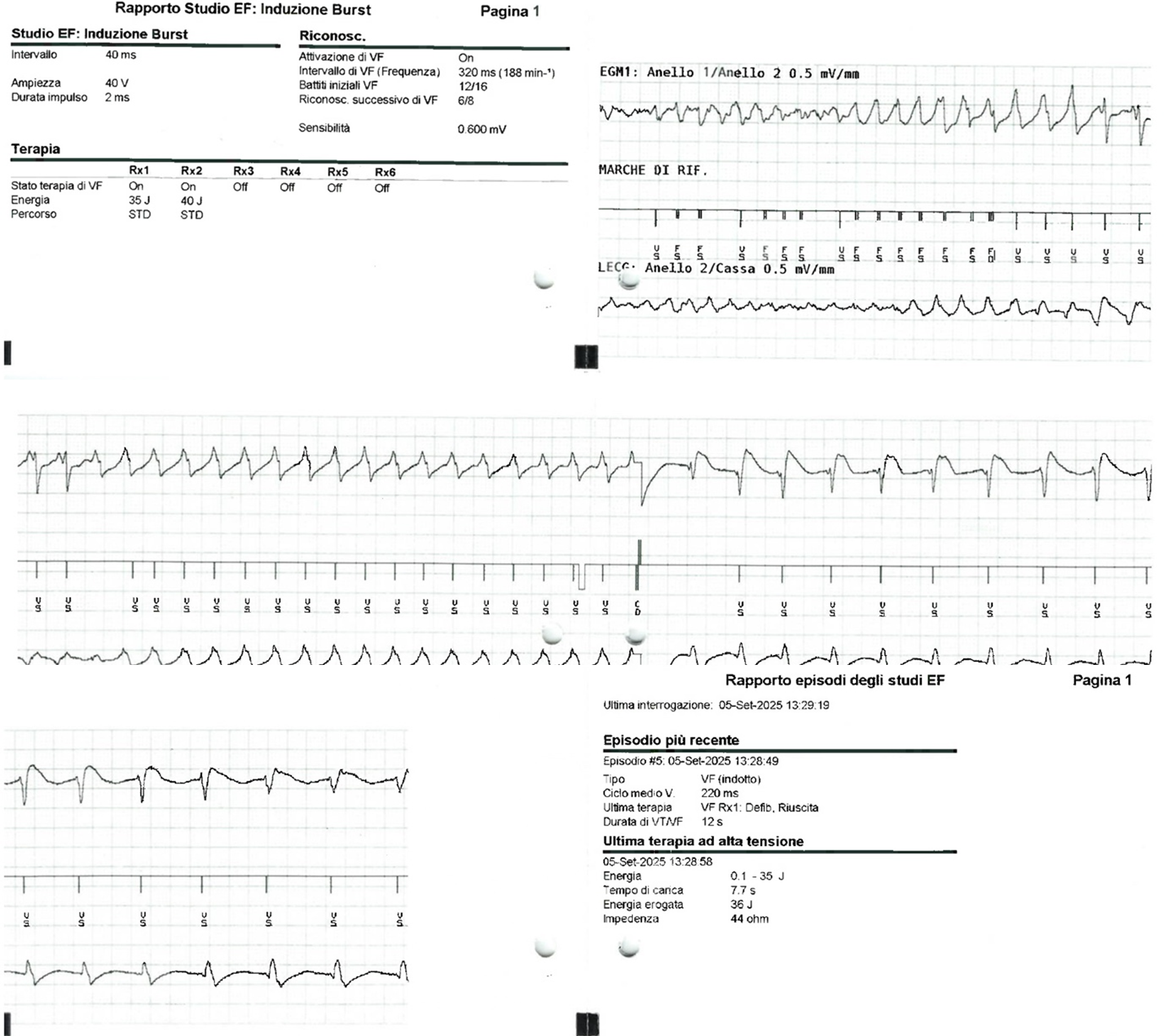
Patient Presentation A 77-years old man with a recent hospitalization for a late presentation myocardial infarction was discharged with a severe compromission of the ventricular ejection fraction. During the cardiovascular rehabilitation he developed an episode of SVT with hemodynamic instability treated with RCP with rapid ROSC. Then he accessed to our emergency department for further investigations. Initial Work-Up The thoracic CT scan showed costal and sternal fracture with a retrosternal hematoma. Moreover, due to the long hospitalization, the patient developed a urinary tract infection sustained by Enterococcus faecalis and Klebsiella pneumoniae. Taking into account that a previous CT scan showed an extensive diverticular disease of large intestine with high risk of bacterial translocation, a specific antibiotic therapy was administered until negative blood and urinary cultures resulted. Admitted to our CVICU, the initial work up was performed by CMR which showed up a biventricular disfunction (LVEF 36%, RVEF 39%) with the presence of transmural LGE of inferior wall and infero-lateral wall of the left ventricle and inferior and lateral wall of the right ventricle. Diagnosis and Management In consideration of the infection risk, the transvenous ICD was not the preferable choice and the SVT nature with a diffuse transmural LGE made the S-ICD not the desirable device. The standard EV-ICD positioning was not deemed achievable in consideration of the presence of retrosternal hematoma and sternal fracture. The case was discussed in Heart Team and a surgical approach was proposed to overcome these issues. Via full sternotomy and with beating heart the EV-ICD was implanted following the evacuation of the hematoma. The catheter was positioned fully intrathoracically in order to reduce the risk of rupture and infection. Then, it was directly sutured on the pericardium and t he sternal fracture reduced during the standard sternal closure with steel wires. Conclusions This case has highlighted the feasibility of a totally surgical and intra-thoracic EV-ICD implantation, representing a further step into prevention of SCD when other ICD devices implants are not feasible. More data are needed regarding the efficacy of this technique, as well as long-term data on lead parameters and ICD performance, to consider this procedure as an alternative to traditional ICDs implantation.