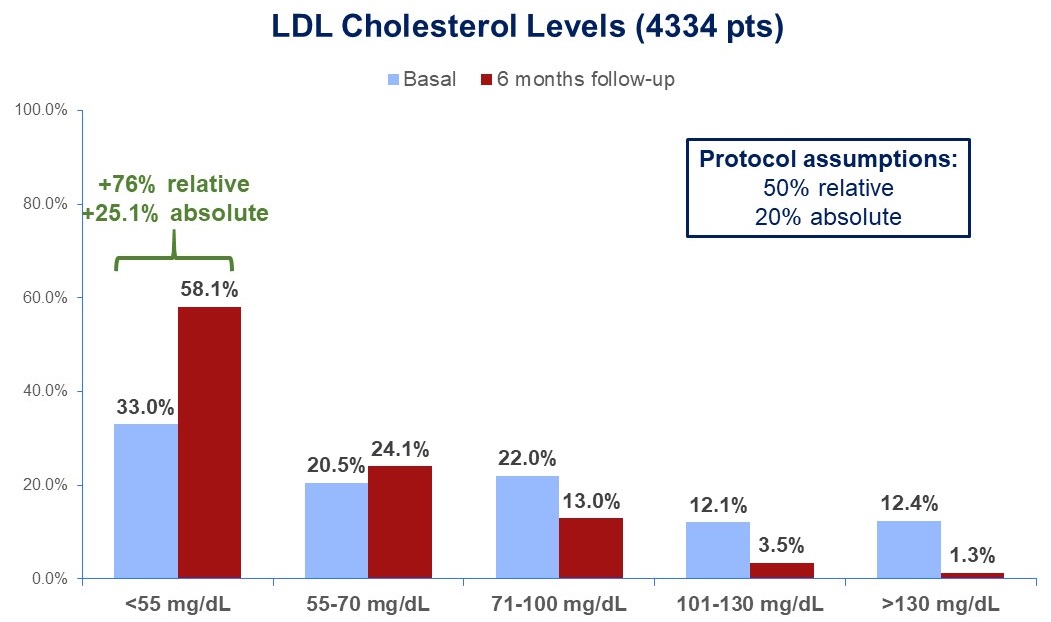
Background. Adherence to guideline recommendations for secondary prevention strategies appears to be largely inadequate. Aim. To try to narrow the gap between what is recommended and what is implemented in clinical practice, we designed a national implementation science project, BRING-UP Prevention, based on educational programmes and patient data collection. Methods. BRING-UP Prevention is a nationwide, observational, prospective, multicentre study enrolling patients with a documented prior atherothrombotic event. The study consists of two 3-month enrolment phases followed by a 6-month follow-up with end-point evaluation, with each enrolment phase preceded by an educational intervention to discuss guideline recommendations. These data refer to the primary endpoint, which was the percentage of patients achieving the target LDL cholesterol level of <55 mg/dL. The first phase has recently been completed. Results. Over 3 months, 189 cardiology centres collected data on 4790 patients, 2500 discharged from hospital and 2290 managed as outpatients. Follow-up data at 6 months were available for 4643 patients (96.9%). The rate of patients with LDL cholesterol <55 mg/dL increased from 33% to 58.1%, with absolute and relative increases of 25.1 and 76.0%, respectively. Overall, the proportion of patients with LDL cholesterol ≤70 mg/dL increased from 53.5% to 82.2%. At discharge/end of visit, 96% of patients were on statins and 94.7% were still on statins at 6 months. Atorvastatin and rosuvastatin were the most commonly prescribed statins, in more than 75% of cases at high doses. Ezetimibe was prescribed in 84% of cases. The figure shows LDL cholesterol levels at baseline and after 6 months of follow-up. PCSK9Is were prescribed in 7.7% and inclisiran in 2.3% of patients. Pts with partial or total intolerance to statins were 4.5%. Conclusions. Data from the first phase of the BRING-UP Prevention study show that: 1) the rate of pts with LDL cholesterol level <55 mg/dL increased consistently over the 6-month follow-up period; 2) this result was achieved with high intensity statins, often in combination with ezetimibe, while the use of new lipid-lowering drugs remained limited. These data show that it is possible to significantly increase the percentage of patients achieving guideline-recommended LDL cholesterol levels with a very favorable cost-benefit approach using a high-intensity statin in combination with ezetimibe.