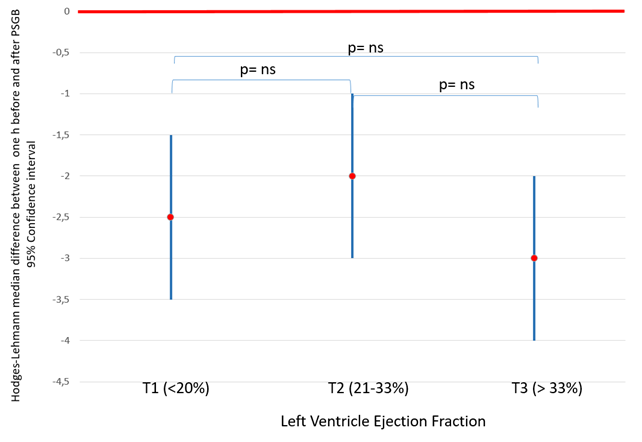
Introduction Percutaneous stellate ganglion block (PSGB) modulates sympathetic nervous system activity and has proved to be both effective and safe in the treatment of ventricular arrhythmic storms. While observational studies on large cohorts have highlighted its efficacy, it remains unclear whether its effect and safety are influenced by the degree of left ventricular dysfunction. Materials and Methods This analysis included the PSGB procedures performed between July 1, 2017, and April 30, 2024, in the 19 Italian centres participating in the STAR project. Procedures were categorized into three groups based on the tertiles of left ventricular ejection fraction (LVEF) before the procedure: T1: LVEF < 20%, T2: LVEF 20%-33%, and T3: LVEF > 33%. For each group, the number of shocks (external or internal) and antitachycardia pacing (ATP) interventions during the hour before and the hour after the PSGB was compared. The extent of reduction in treated events was analyzed across groups. Results A total of 180 patients underwent 254 PSGB procedures, with pre-procedure LVEF data available for 244 cases [T1: 84 (34%); T2: 82 (34%); T3: 78 (32%)]. The procedures resulting in a complete arrhythmic suppression within the first hour after PSGB was similar among groups (T1: 82%, T2: 86%, T3: 89%, p=0.39). In all three groups, PSGB led to a significant reduction in the number of shocks and/or ATP interventions during the first hour post-procedure compared to the hour before [T1: 2 (1–3) vs. 0 (0–0), p<0.01; T2: 2 (1–3) vs. 0 (0–0), p<0.01; T3: 2 (1–4) vs. 0 (0–0), p<0.01], with the extent of reduction being similar among groups (Figure 1). Furthermore, LVEF was not associated with the likelihood of complete arrhythmic suppression in the hour following PSGB [T1: reference; T2: OR 1.4 (95% CI: 0.6–3.2),p=0.45; T3: OR 1.9 (95% CI: 0.7–4.7), p=0.18]. The complication rate was low and comparable among the three groups (T1: 0%, T2: 1.2%, T3: 0%, p=0.37). Conclusions Our study confirms that PSGB is effective in reducing the number of shocks and/or ATP interventions in patients experiencing electrical storms, regardless of the extent of left ventricular dysfunction. This is particularly significant as PSGB can be safely used even in patients with severe left ventricular dysfunction.