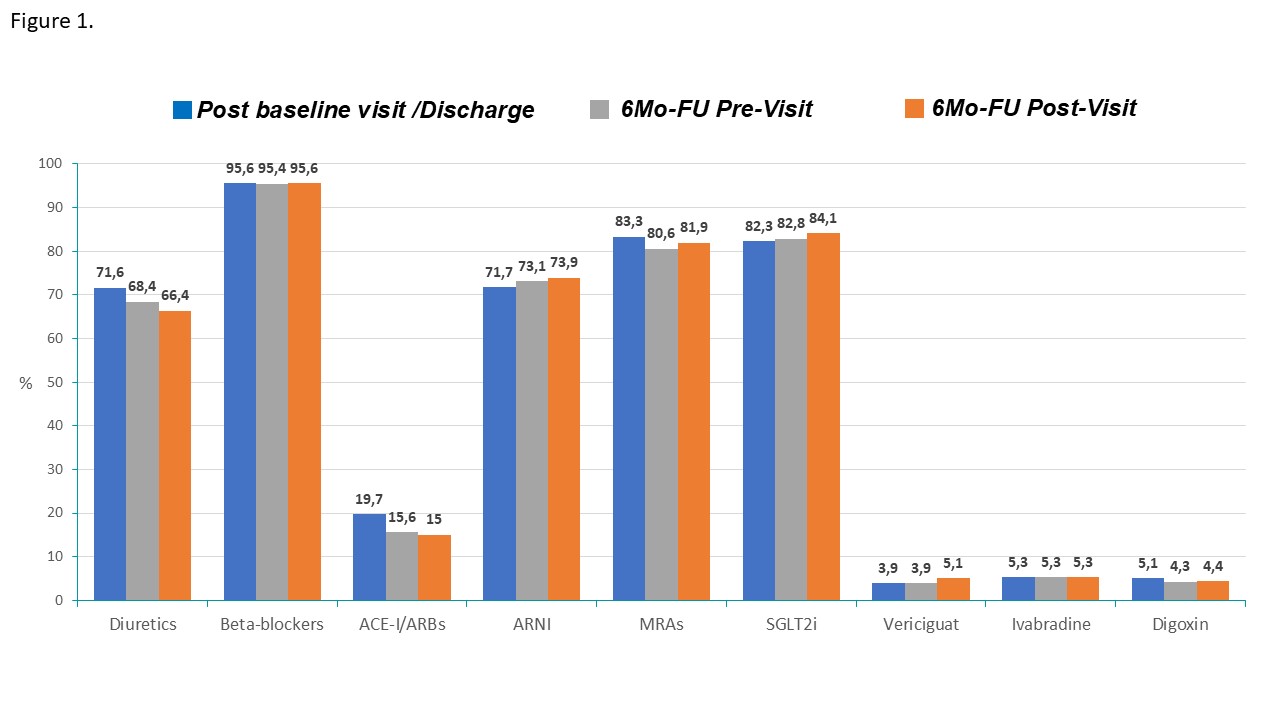
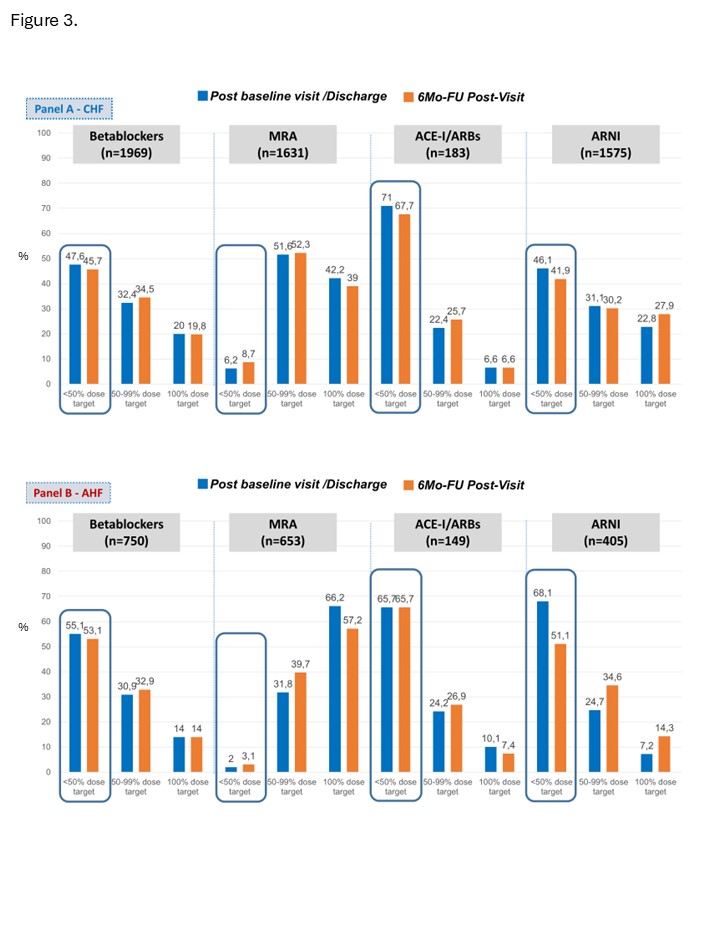
Background: Current ESC guidelines introduced a four-pillar approach for the treatment of HFrEF. Nevertheless, there is limited data regarding implementation, up-titration and discontinuation of recommended medical treatments in clinical practice. Objectives: BRING-UP-3 Heart Failure (HF) study was designed to evaluate the Guideline recommendations implementation in HF patients enrolled by a large sample of Italian cardiology sites. Methods: BRING-UP-3 HF study is an observational, prospective, nationwide investigation encompassing 179 sites enrolling ambulatory and hospitalized HF patients. The study includes an educational intervention followed by two three-month enrollment periods and by a six-month follow-up period with end-point evaluation. For HFrEF patients, the objective is to describe the proportion of patients who receive the four pillars. This analysis focuses on HFrEF patients enrolled in the ambulatory and hospitalized cohorts with medical treatment data available at six months follow-up. Results: Of the 3,201 HFrEF patients enrolled in the study, 142 had died and medical treatment data was available for 2950 patients at six months. The mean age was 69±11 years (26.6% over 75 years), females were 18.0%. Prescription rates of main HF medications at baseline and 6-months are shown in Figure 1. Prescription rates of the 4 pillars were high at baseline and remained overall stable during the six months follow-up with a decrease of ACE-I/ARBs in favor of ARNIs, a small increase in SGLT2i and a decrease in the prescription of diuretics (not prescribed to one third of the patients). Combination therapy of recommended treatments also remained stable at six months (Figure 2) with quadruple therapy prescribed in 64.3% of patients at six months (vs 63.9% prescription at the baseline visit/discharge). Six-months dose up-titration remained suboptimal both for patients enrolled in the acute (Figure 3, Panel A) and in the ambulatory settings (Figure 3, Panel B) with most treatments prescribed at less than 50% of recommended dose. Discontinuation rates at six months follow-up were very low: 1.5% for Betablockers, 7.0% for MRAs, 4.6% for SGLT2i, 3.5% for ARNIs and 26.9% for ACE-I/ARBs (mostly due to a shift to ARNIs). Conclusions: A comprehensive analysis of a large sample of Italian cardiology sites revealed a high persistence of guideline-recommended treatments at six months with low rates of discontinuation while dose up-titration remains suboptimal.