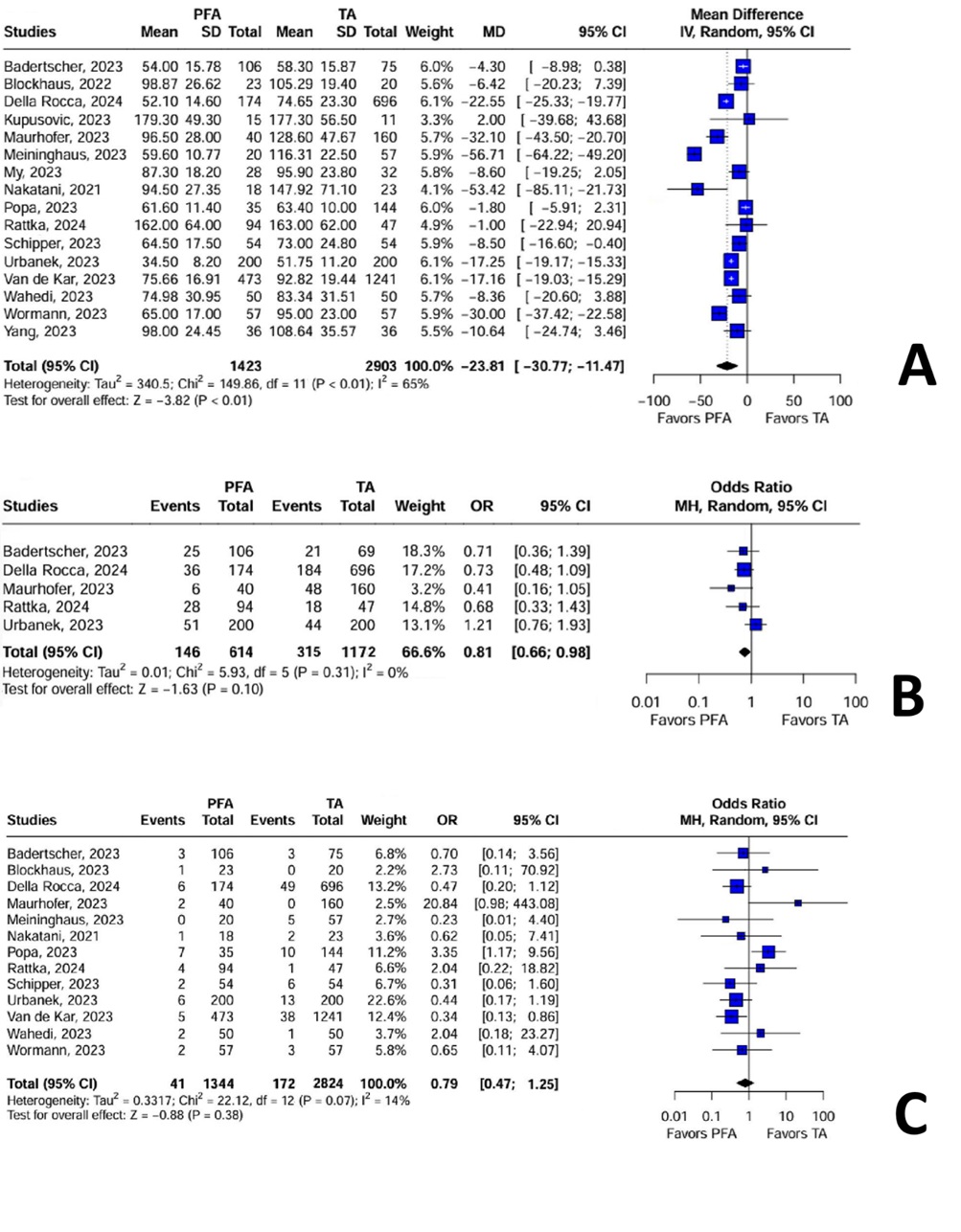
Background: Recent randomized clinical trials (RCTs) on pulsed-field ablation (PFA) systems for treating atrial fibrillation (AF) have shown promising potential to reduce complications associated with conventional thermal modalities while maintaining efficacy. However, RCT results may not fully reflect real-world clinical practice. Objective: This study aims to compare the safety and efficacy of PFA and thermal ablation (TA) in real-world settings through a meta-analysis of published observational studies. Methods: Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, we searched Medline, Embase, and Scopus to identify all observational studies published up to October 2024 comparing PFA and TA in patients with AF undergoing their first catheter-based therapy for pulmonary vein isolation. Weighted mean differences (MDs) were used to pool continuous outcomes, while treatment effects for binary outcomes were compared using odds ratios (ORs) with 95% confidence intervals (CIs), applying a random-effects model (DerSimonian-Laird method). Heterogeneity was assessed using the Higgins I² statistic. Results: Sixteen studies involving 4,326 patients [1,423 (32.8%) treated with PFA] were included. PFA was associated with a shorter procedure time compared to TA (MD: -23.81; 95% CI: -30.77 to -11.47). Additionally, PFA demonstrated a lower treatment failure rate after one year of follow-up (OR: 0.81; 95% CI: 0.66 to 0.98, I²: 0%) and no significant differences in overall periprocedural complications compared to TA (OR: 0.79; 95% CI: 0.47 to 1.25, I²: 14%). Conclusion: PFA is significantly associated with shorter total procedure times and lower rates of AF recurrence one-year post-procedure compared to TA, with similar risks of periprocedural complications.