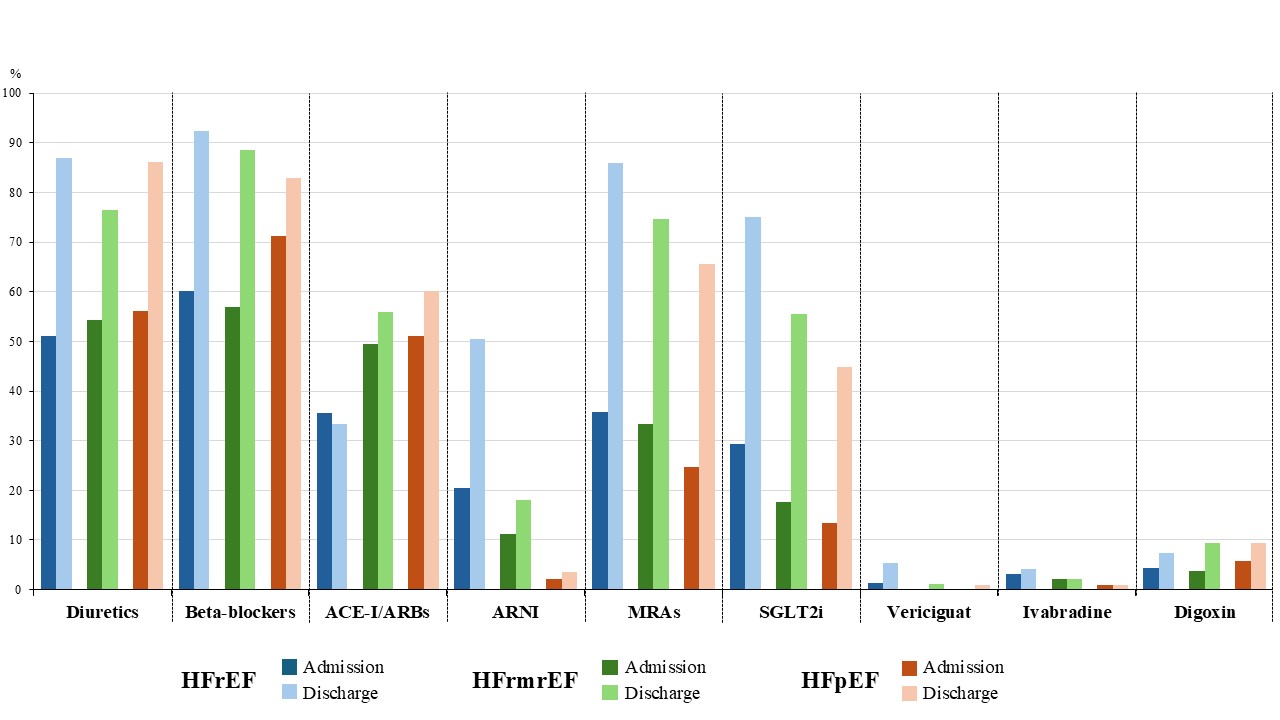
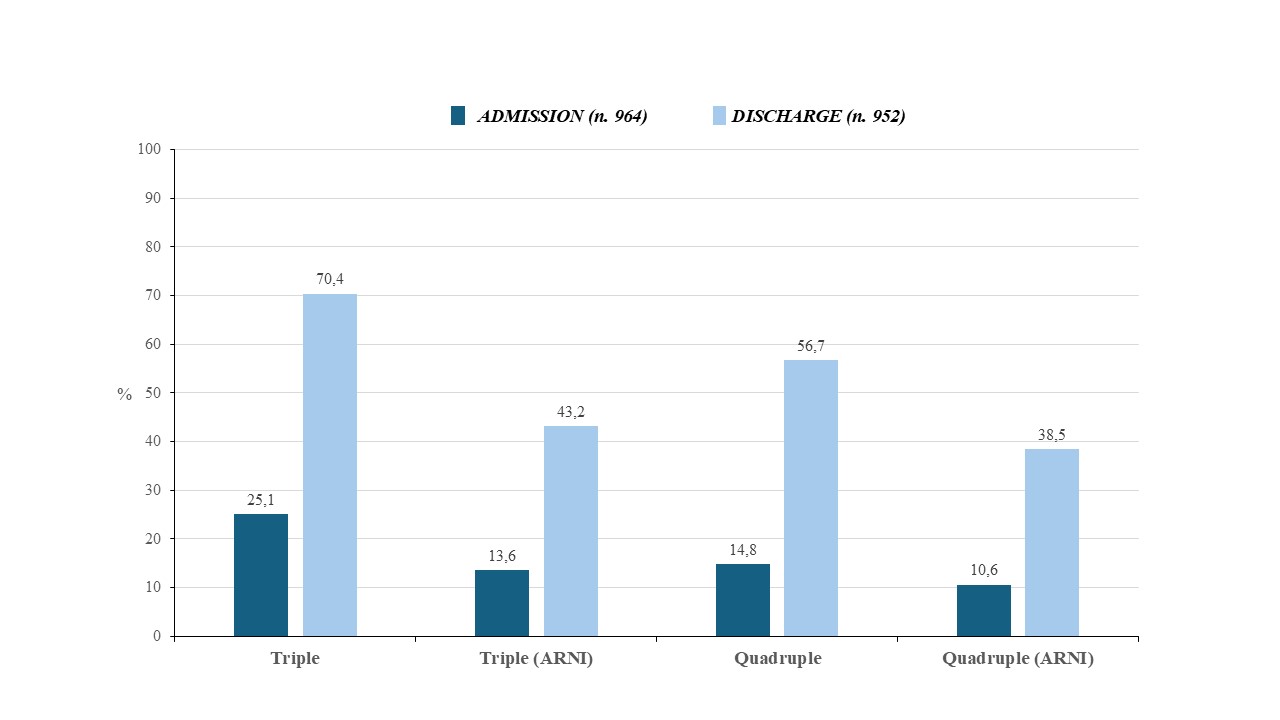
Background: Recent ESC guidelines introduced a new treatment paradigm for HFrEF, with a novel four pillar therapeutic approach comprising ACE-I/ARBs/ARNIs, Beta-blockers, MRAs, and SGLT2i. Furthermore, these guidelines for the first time give a Class IA recommendation for Empagliflozin and Dapagliflozin in HFmrEF and HFpEF. Evaluation of transferability of RCTs derived evidence to clinical practice and guideline recommendation implementation are two major issues. Hospital admission is considered an important chance for treatment optimization. Aims: To describe discharge treatments of acute heart failure (AHF) patients enrolled by Italian cardiology sites participating to the nationwide BRING-UP3 HF study. Methods: BRING-UP-3 HF study is an observational prospective, nationwide investigation involving 179 sites and enrolling ambulatory or hospitalized HF patients in two three-month periods, followed by a six-month follow-up with end-point evaluation. For HF with reduced ejection fraction (HFrEF), the objective is to describe the prescription rate of the four pillars. Baseline enrollment data for the hospitalized cohort (Phase I) are here presented. Overall, 1373 patients were included. Mean age was 71±12 years (40.6% 75+ years) and 29.8% were females. A high percentage of patients (42.7%) had de novo HF. Patients with HFrEF were prevalent (70%), followed by HFpEF (16%) and HFmrEF (14%). History of hypertension, atrial fibrillation, diabetes mellitus, and chronic kidney disease was reported in 74.7%, 43.3%, 34.6%, and 32.6%, respectively. Medical treatment prescription on admission and at discharge among different groups of patients are shown in Figure 1. In HFrEF patients, an increase from the admission to discharge prescriptions of beta-blockers (60.1% to 92.4%), RASi (56% to 83.7%, with ARNIs preferred over ACE-I/ARBs), MRAs (35.8% to 86%) and SGLT2i (29.3% to 75.0%) was observed. These prescription rates resulted in a high prescription of combination treatments with 56.7% receiving the four therapeutic pillars at discharge (Figure 2). Among HFmrEF and HFpEF patients, prescription rates of SGLT2i reached 55.5% and 44.8%, respectively. Conclusions: A comprehensive analysis of a large sample of Italian cardiology centers revealed a high discharge prescription rate of guideline-recommended treatments across ejection fraction phenotypes.