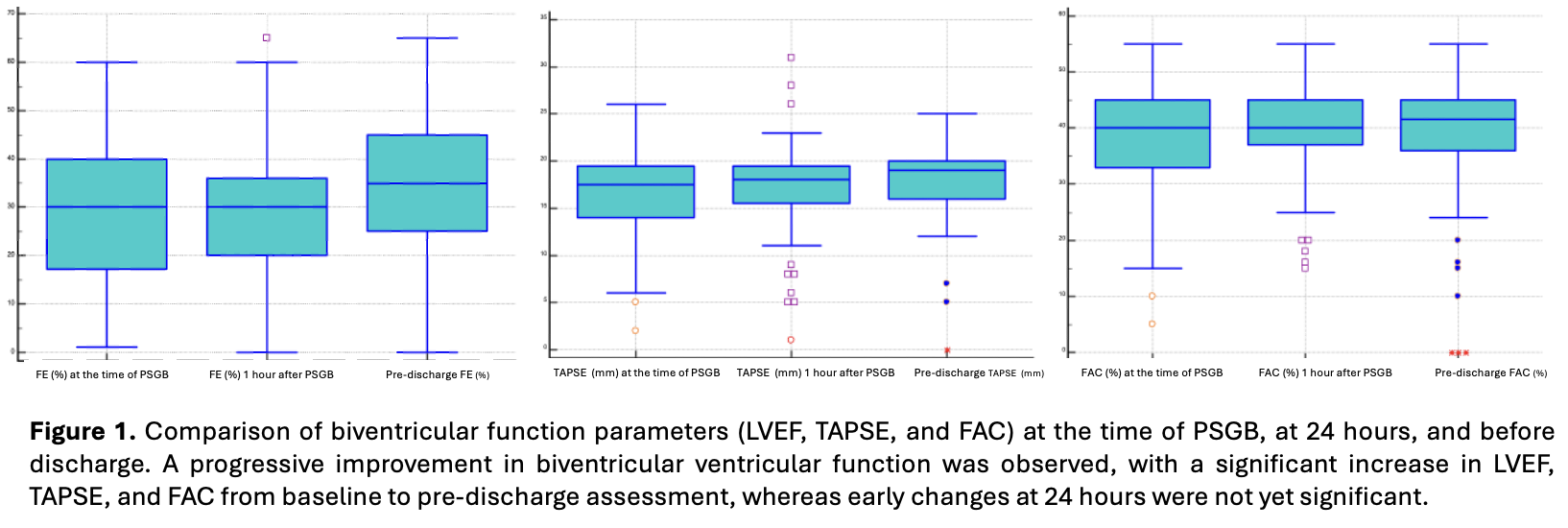
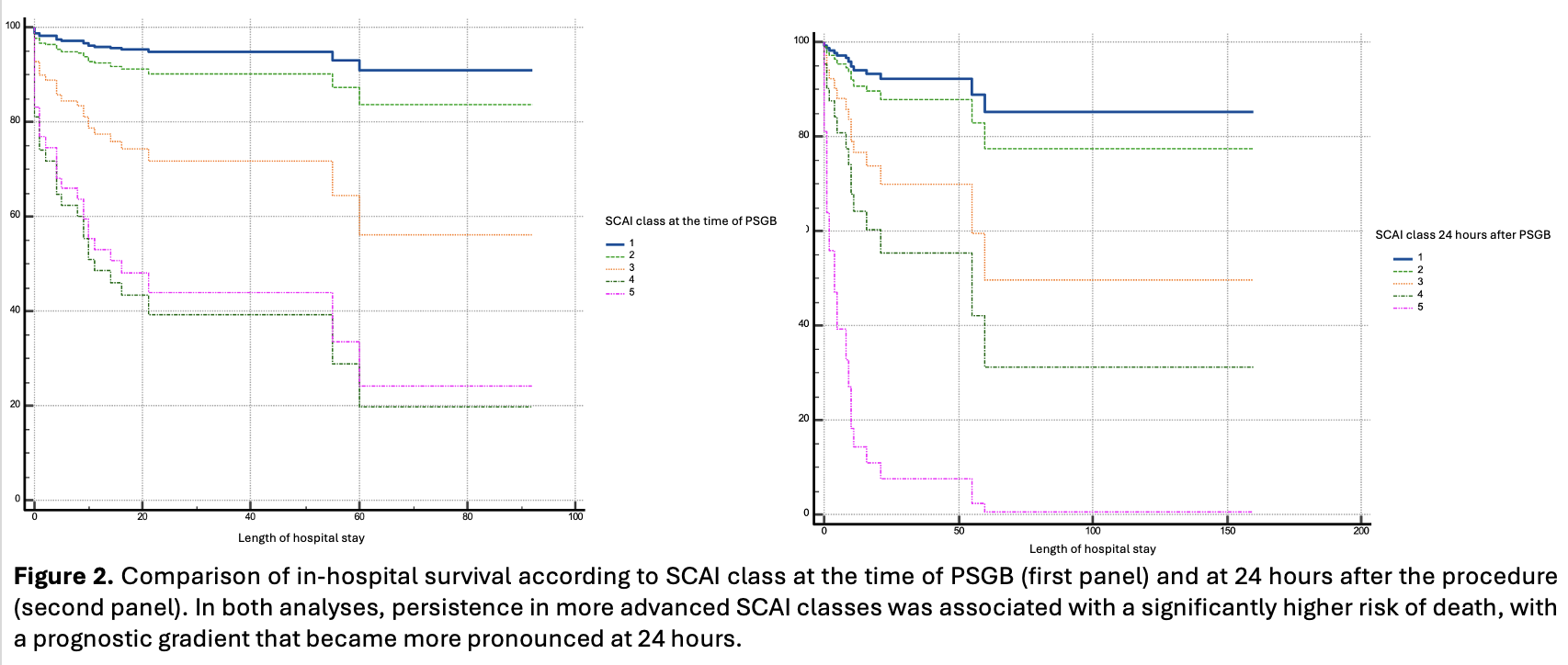
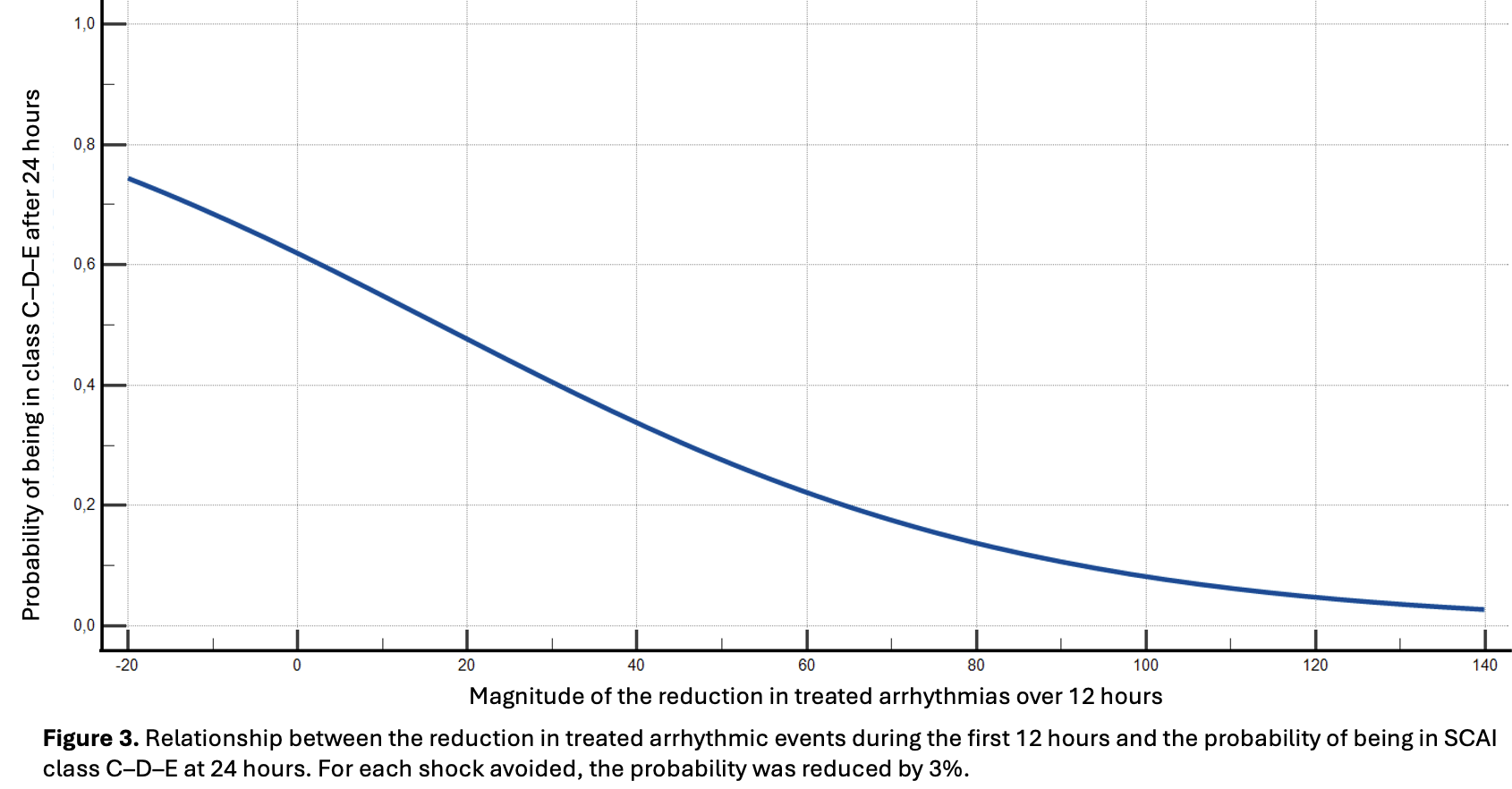
Introduction . Electrical storm (ES) complicated by cardiogenic shock (CS) is a life-threatening emergency sustained by the interaction between malignant ventricular arrhythmias (VA), hemodynamic deterioration, and sympathetic hyperactivation. Percutaneous stellate ganglion block (PSGB) has emerged as a neuromodulatory strategy to interrupt this vicious cycle. We performed a retrospective analysis of the prospective multicenter STAR registry. Aims . To evaluate the impact of PSGB on cardiac function, hemodynamic profile, and clinical outcomes in patients with ES complicated by CS. Materials and methods . We analyzed 115 PSGB procedures performed from July 2017 to August 2025 in patients with ES and CS of different etiologies (ischemic heart disease: 37.4%) across 10 Italian centers. The primary endpoint was the impact of PSGB on hemodynamic profile, defined by SCAI class, lactate clearance, and biventricular systolic function. Secondary endpoints included antiarrhythmic efficacy and the association between SCAI class and in-hospital mortality. Results . The study population was predominantly male (76%), with a median age of 68 years (IQR 57–79). Within 24 hours after PSGB, the proportion of patients with severe CS (SCAI class C–D-E) significantly decreased (47.8% vs 29.2%, p<0.0001), along with median lactate levels (2.02 vs 1.03 mmol/L, p=0.0003). Left ventricular ejection fraction improved from PSGB to discharge (30% to 35%, p<0.0001), together with right ventricular function [FAC 40% to 42%, p=0.02; TAPSE 18 to 19 mm, p=0.016], while early 24-hour changes were not significant. SCAI class independently predicted in-hospital mortality at baseline and at 24 hours (all p<0.05). PSGB was associated with a marked reduction in ventricular arrhythmic events (3 [1–7] vs 0 [0–1] in the 12 hours pre- vs post-PSGB, p<0.0001), already evident within 1 hour. Greater arrhythmia reduction was associated with a lower probability of severe CS at 24 hours (OR 0.97 [0.94–0.99], p=0.03). Conclusions . PSGB was safe and highly effective in suppressing refractory VA, improving hemodynamic stability, and enabling progressive ventricular recovery. These findings support PSGB as a valuable therapeutic option in ES complicated by CS and highlight the prognostic relevance of early post-procedural SCAI class.