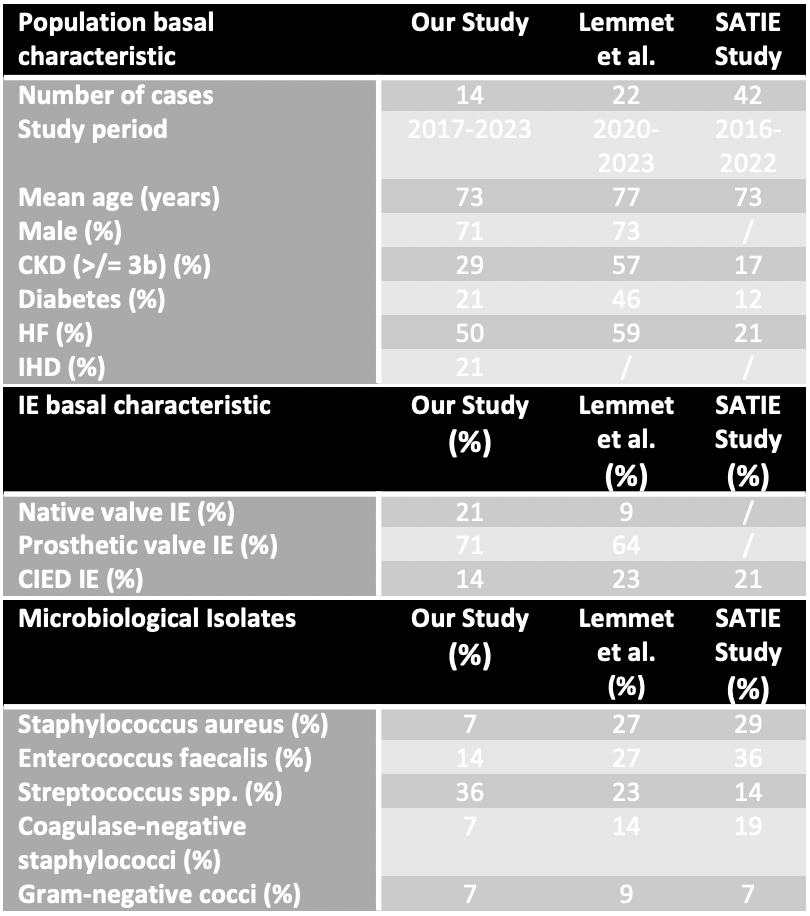
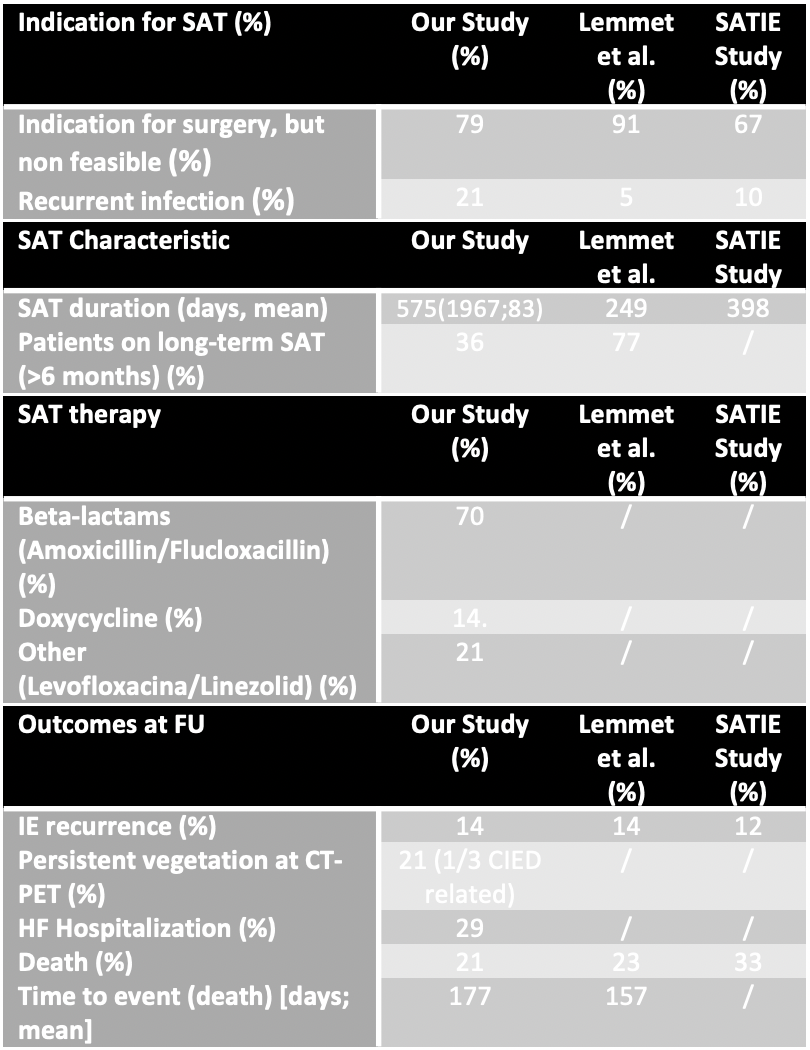
Background and aim Suppressive antibiotic therapy (SAT) is a palliative, non-curative approach for managing infective endocarditis (IE) in selected patients. This retrospective observational descriptive study aimed to evaluate the efficacy and safety of SAT in IE patients ineligible for cardiac surgery. Methods We analyzed 14 IE patients treated with SAT between 2017 and 2023, selected from a cohort of 129 IE cases diagnosed according to ESC 2023 guidelines of which detailed data were collected. Follow-up was defined as the period from the transition from curative parenteral therapy to SAT until death or the most recent follow-up date. Results The study cohort primarily comprised elderly males with significant comorbidities such as diabetes, heart failure, and chronic kidney disease. Prosthetic valve IE was most common, predominantly affecting biological valves (42% aortic, 29% mitral). Native valve and CIED IE were less frequent. Streptococcus species were the main pathogens identified. SAT lasted an average of 575 days, with 36% of patients on long-term therapy. Beta-lactams were the primary antibiotics used. The study reported a 14% IE recurrence rate and 29% mortality rate, with a mean time to all-cause death of 177 days. These findings align with recent studies, (SATIE study and Lemmet et al.'s research): in fact the observed outcomes suggest effective management of this high-risk population, and, comparatively, the extended mean SAT duration indicates good tolerability in selected inoperable IE patients with multiple comorbidities and high surgical risk. Discussion and conclusion Recent guidelines recognize SAT as a potential strategy for IE patients ineligible for cardiac surgery. However, they highlight the lack of robust evidence supporting its efficacy and provide no specific protocols. Despite limitations such as small sample size, retrospective design, and absence of a control group, our preliminary findings, in line with existing literature, suggest potential efficacy and safety of SAT in selected high-risk IE cases with limited treatment options. Future research should focus on determining optimal SAT duration, clarifying its role in specific patient populations (especially those with CIED-related IE), and evaluating advanced imaging modalities like PET/CT for assessing recurrence rates and guiding follow-up management. These efforts will contribute to developing more comprehensive, evidence-based guidelines for SAT use in IE management.