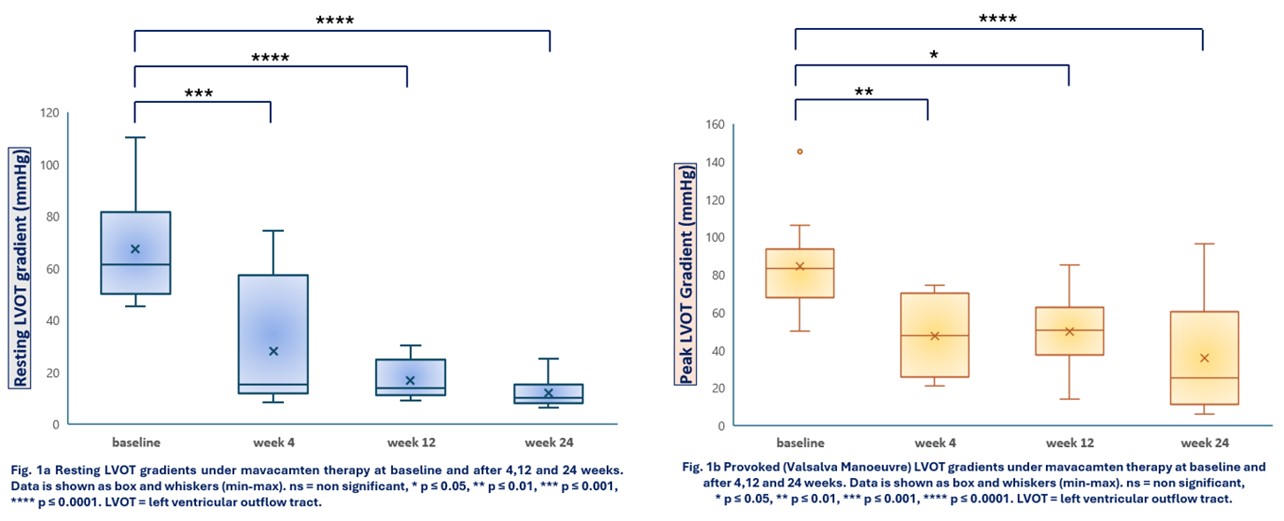
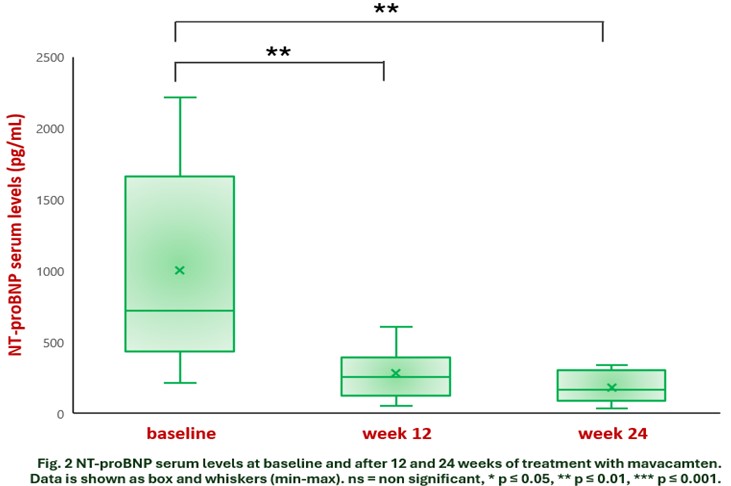
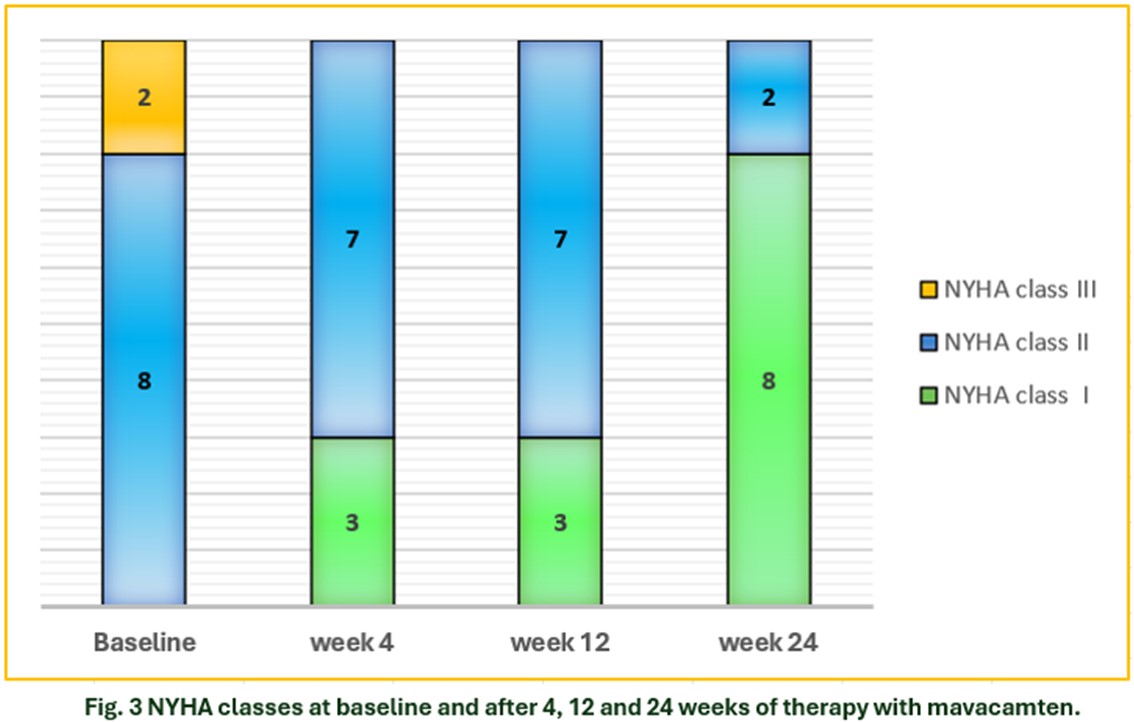
Introduction: Mavacamten, a first-in-class cardiac myosin ATPase inhibitor used as second-line therapy for hypertrophic obstructive cardiomyopathy (HOCM), became available in Italy in early 2024 under a compassionate use program. Aim: To describe early experience of compassionate use of Mavacamten in a single centre HOCM population. Methods: All patients had a peak LVOT gradient ≥ 50 mmHg, either at baseline or provoked, a LVEF ≥55% and were symptomatic at the highest tolerated dose of first-line drugs. Genotyping for cytochrome P450 (CYP2C19) was performed to determine the correct starting dosage of Mavacamten. Periodic clinical evaluation, ECG, cardiac imaging, laboratory work-up were assessed as per compassionate use protocol. Dosing of mavacamten was adjusted according to manufacturer’s recommendations. Results: Mavacamten was started in 11 patients (72% male, age 55.9 ± 16, NYHA class II 72.7%, NYHA class III 27.3%, mean HCM risk score 3.1±1.26), none of them with a slow metabolizer profile. On December 2024, 10 of the 11 enrolled patients completed the 24-week (W) follow-up (FU) assessment that revealed a statistical significant reduction of LVOT gradients and NT-proBNP serum levels. Mean resting and provoked (Valsalva Manoeuvre) LVOT gradients decreased, respectively, from 67.1 ± 21.5 mmHg and 84.4 ± 26.8 mmHg at baseline to 11.8 ± 5.7 mmHg and 35.7 ± 30.4 mmHg at 24 W, with mean changes of 55.3 ± 18.7 mmHg (95% CI [41.8; 68.7], p < 0.0001) and 48.7 ± 16.3 mmHg (95% CI [37; 60.3], p < 0.0001) (Fig.1a-1b) . Mean NT-proBNP serum levels significantly decreased from 907.6 ± 691.3 pg/mL (baseline) to 153.3 ± 112.9 pg/mL (24 W), with mean changes of 754.2 ± 620.6 pg/mL (95% CI [310.2; 1198.2], p = 0.004) (Fig. 2). All patients reported an improvement of at least one NYHA class at 24W FU (Fig.3). Mavacamten was up-titrated to 10 mg/die (6 patients) and 15 mg/die (4 patients) regimen therapy with no case of LVEF < 55%, nor any other major adverse events requiring discontinuation of treatment. Conclusions: We provide first insights into the usage of Mavacamten in HOCM patients in a real-world setting. In a small cohort of symptomatic patients with HOCM, treatment with mavacamten, in combination with first-line therapies, was effective in reducing both baseline and latent LVOT obstruction. A favorable impact was also observed on laboratory parameters and quality of life, without any major adverse events requiring discontinuation of the treatment.