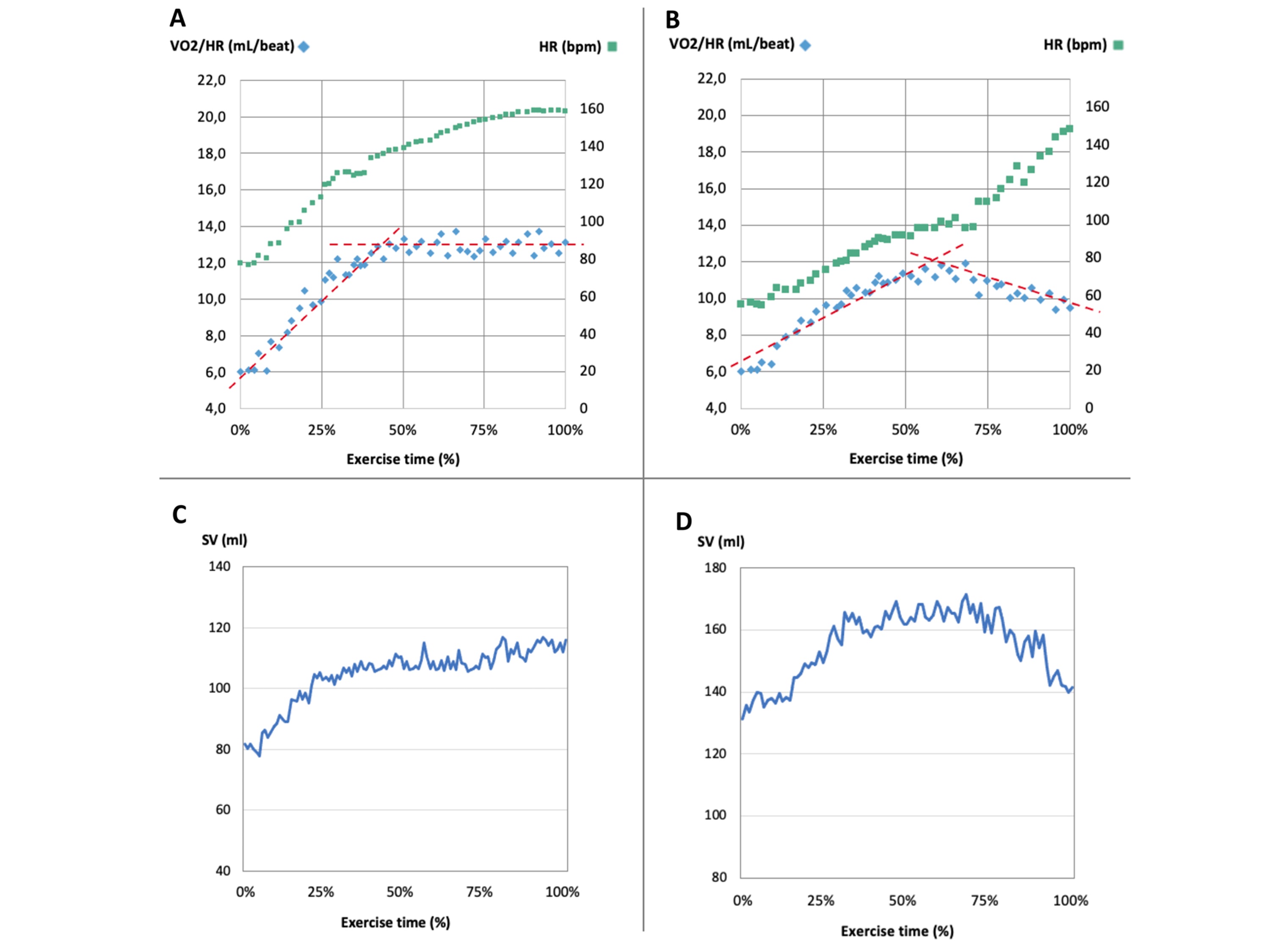
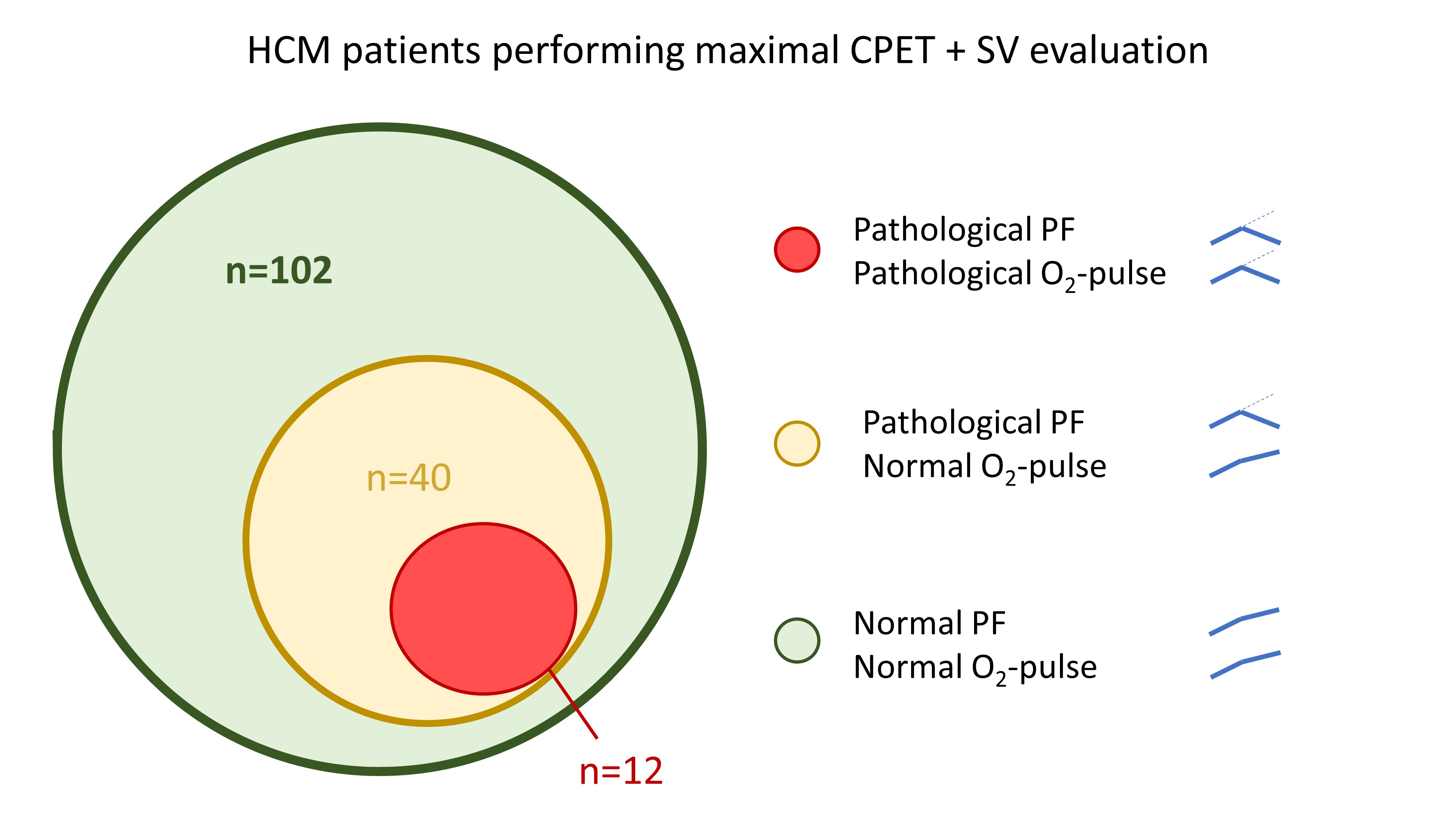
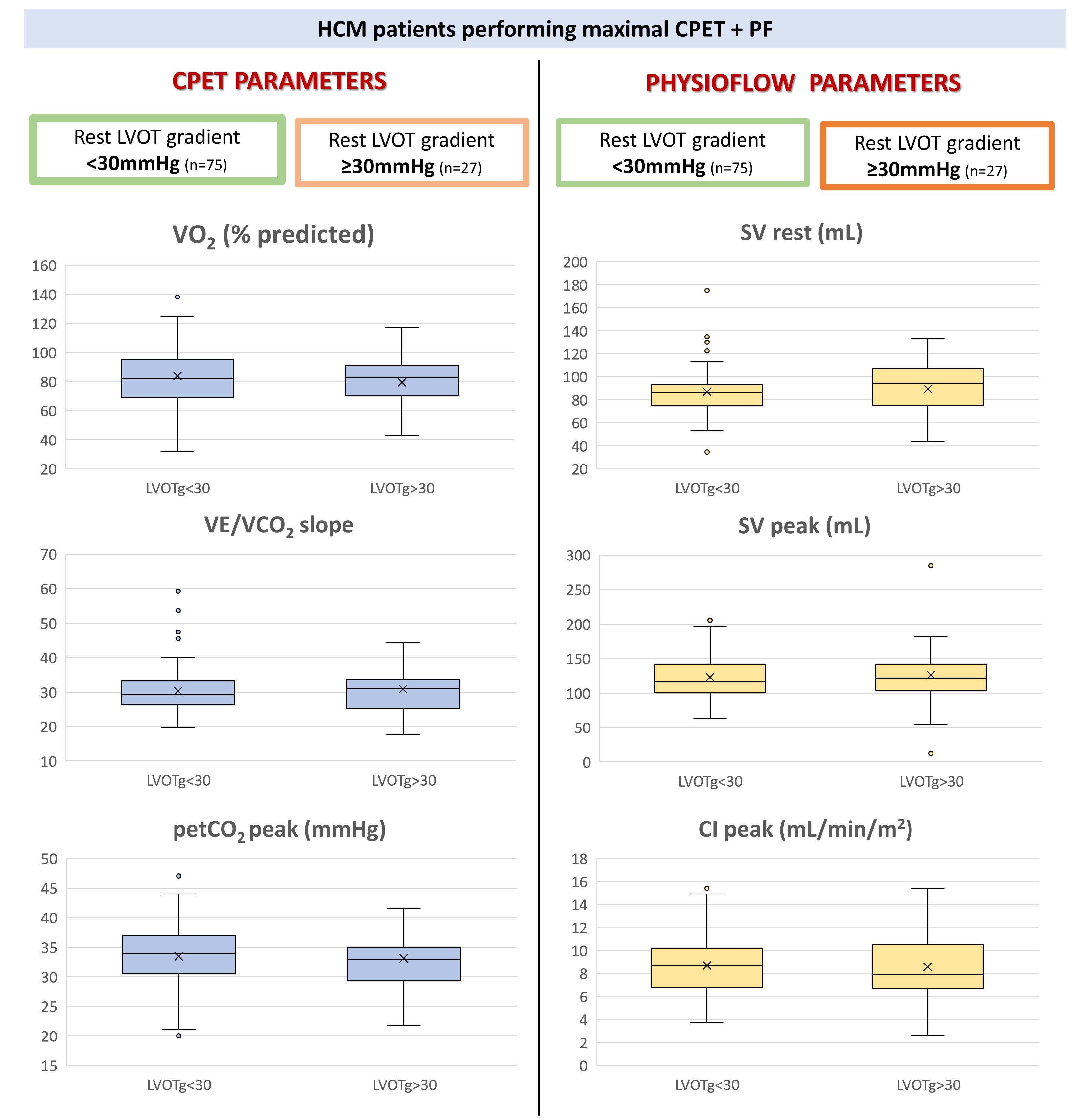
Background: in hypertrophic cardiomyopathy (HCM), cardiopulmonary exercise testing (CPET) is the gold standard for evaluating impaired exercise tolerance. The O2-pulse is calculated as oxygen uptake/heart rate, and it is used as a surrogate for stroke volume (SV). Abnormal O2-pulse kinetics suggests inadequate SV increase. Research question: since reduction of SV may be overcome by O2 extraction increase, a direct non-invasive SV measurement is desirable. Methods: 102 HCM patients (53±16 years, 78% male) with predominantly non-obstructive phenotype (74%) underwent CPET with SV measurements by Physioflow® (PF). Results: No significant CPET differences were noted regarding the presence of left ventricular outflow tract obstruction. Abnormal O2-pulse kinetics were found in 12 patients, all paralleled by abnormal SV changes by PF. Differently, PF identified 28 additional patients with abnormal SV trends. Abnormal SV kinetics were associated with higher peak VE/VO2 ratio (42.6 [37.4–47.5] vs. 38.0 [33.6–41.3]) and lower end-tidal CO2 values (PetCO2) (31.8±4.9 mmHg vs. 34.3±5.6 mmHg) (p< 0.05 for both). The patients with greater SV growth in the last 25% of exercise showed not significant peakVO2 differences, but, VO2 at anaerobic threshold (49.8±12.3% of predicted peakVO2 vs. 43.9±15.2%), VO2/work slope (10.2±2.0 mL/min/Watt vs 9.3±1.3 mL/min/Watt) and peak PetCO2 (34.5±5.6 mmHg vs. 32.3±5.2) higher, while VE/VCO2 slope (28.7 [24.9–31.0] vs. 31.3 [27.3–34.2] was reduced (p<0.05 for all). Interpretation: The combination of PF and CPET in patients with HCM better identifies patients with abnormal SV kinetics than O2-pulse analysis. The presence of altered SV kinetics is associated to patients’ lower functional capacity.