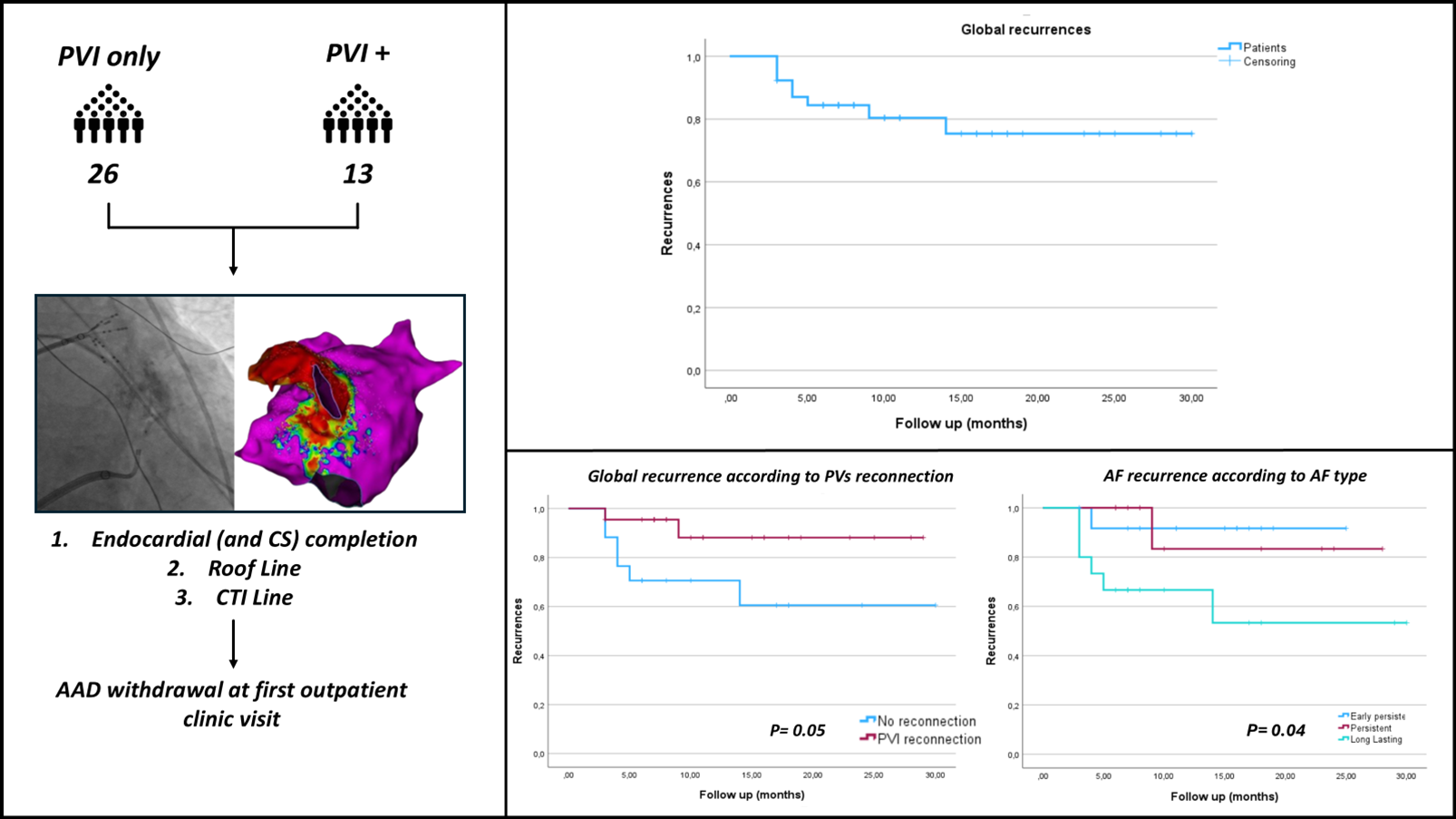
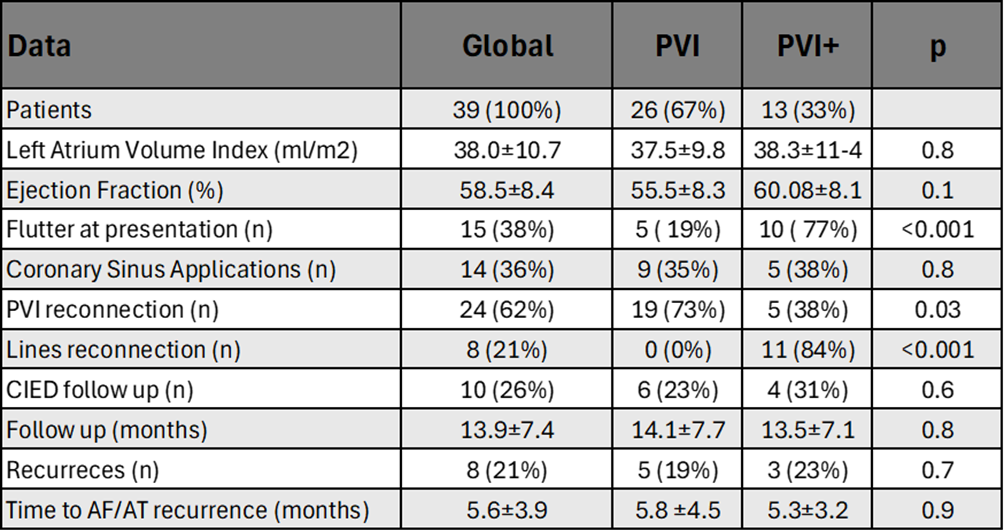
Introduction Procedural strategy for repeated ablation in persistent atrial fibrillation (PeAF) patients is a great challenge, especially in patients with already isolated pulmonary veins (PVs). Vein of Marshall ethanol infusion (VOM-EI) is a promising but poorly investigated approach for PeAF treatment. In this prospective observational study, we analysed PeAF patients undergoing repeated AF ablation with VOM-EI and a standardized anatomical ablation setup. We aimed to evaluate the outcome of this procedural setup based on the previous ablation strategy. Methods 39 PeAF patients were scheduled for repeated ablation, classified by AF type into early PeAF (≤3 months), PeAF (3-12 months), and long-lasting PeAF (>12 months). Based on prior ablation strategy, patients were grouped into PVI or PVI+ (PVs isolation only vs combined with linear lesions and/or CFAEs abolition). We applied a systematic anatomical ablation setup. After VOM-EI, eventual PVI reconnections were targeted. Bidirectional block across prior ablation lines was assessed and touch-up ablation performed if needed. Ablation of the Left Atrial dome, lateral Mitral Isthmus, and cavo-tricuspid isthmus line were sistematically performed and validated. Antiarrhythmic drugs were ceased after 1 month. The primary endpoint was AT/AF recurrences lasting >30 seconds. Kaplan-Meier analysis with Log Rank test and Cox regression analysis evaluated recurrence based on prior ablation setup and AF phenotype. Results 39 PeAF patients were analysed, 26/39 (67%) were PVI and 13/39 (33%) were PVI+. In accordance with AF duration, 11 patients (27%), 10 (27%) and 18 (46%) were respectively classified as early PeAF, PeAF and long-lasting PeAF. Mean follow-up (FU) was 14.4±7.5 months. 8/39 patients (21%) had recurrence of AF/AT during FU. Recurrences occurred in 5/26 (19%) PVI patients and 3/13 (23%) PVI+ ones (p=0.76). Univariate analysis shows PVs reconnection and long-standing AF as significant determinants of arrhythmic recurrences (p=0.05 and p=0.04). PVI reconnection, especially in the PVI group, was associated with arrhythmias-free outcome (p=0.006). Conclusion Regardless of previous procedural setup, VOM-EI in addition to PVI and anatomical scheme validation represents a valid option in repeated ablation for PeAF patients. Patients with PVI reconnection showed a better outcome compared to those with PVI already obtained. Long-lasting PeAF patients had worse outcome.