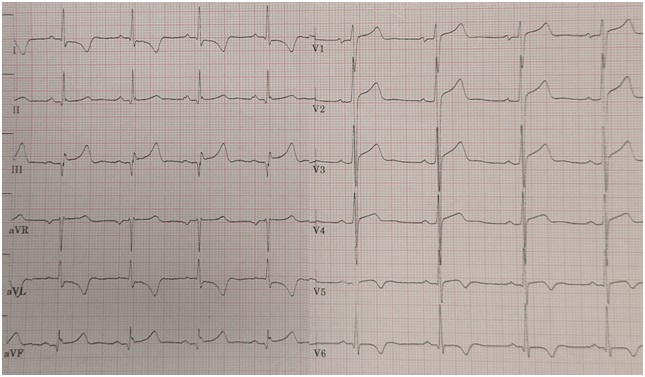
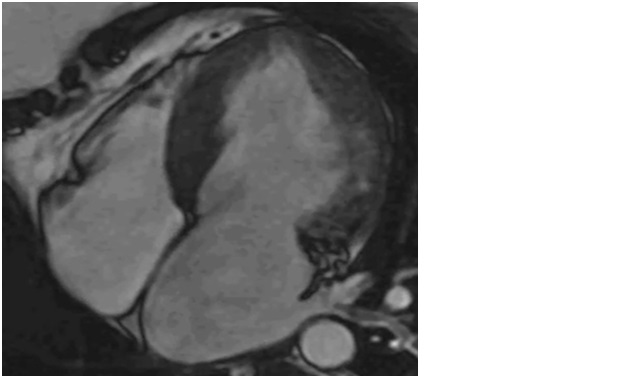
A 36 y.o. man came to medical attention for a screening cardiological examination. The man, who lived in U.S. for 15 years, had returned to Italy to visit his family. He did not report any symptoms or cardiac history. ECG showed Q waves in the inferior leads with elevation of the ST segment and negative T waves in the lateral leads. TTE documented left ventricular symmetric hypertrophy (IVSd 18 mm; PWTd 17 mm), without signs of LVOTO and normal ejection fraction (55%).The patient was referred to our cardiomyopathy clinic: when entered the room, he was noted for wide based and waddling gait. He reported a delay in walking (at 2 years of age), a previous fall trauma with fracture of the upper limb and minor surgery in childhood. Cardiac MRI showed mesocardial LGE at the inferolateral segments, with T2 mapping and native T1 values at the upper limits of normal, and high value in the area of LGE. Genetic testing did not document variants of sarcomeric genes, but given the suspect, a more extensive gene analysis was carried out with detection of the pathogenic variant m.4300A>G in the mitochondrially encoded tRNA isoleucine (MT-TI) gene.Clinical and genetic screening was performed on first-degree relatives: the same mutation was present in the brother (28 y.o.), both with normal cardiac phenotype, and in the mother (57 y.o.) who instead showed left ventricular hypertrophy (LVH) and mesocardial LGE on cardiac MRI, although of a lower degree compared to the proband. The clinical history of the siblings was substantially negative, while the mother reported a form of LVH, previusly attributed to her arterial hypertension; she also had hypothyroidism and a previous clinical diagnosis of polymyositis. Skeletal muscle biopsy performed on the mother demonstrated typical histopathological features of primary mitochondriopathy, allowing to discard the previous clinical diagnosis of polymyositis.Mitochondriopathies are often multisystem diseases, some genetic variants show predilection for a given apparatus such as m.4300A>G mutation of MT-TI gene, which manifests with LVH and skeletal muscle myopathy, tipically with late onset. The variability of the clinical expression of this mutations depends on genetic and environmental factors.Maternal inheritance pattern and characteristics extracardiac manifestations should be a warning signs to consider mitochondriopathies in the diagnostic workup in cases of unexplained LV hypertrophy, not only in newborns and infants.