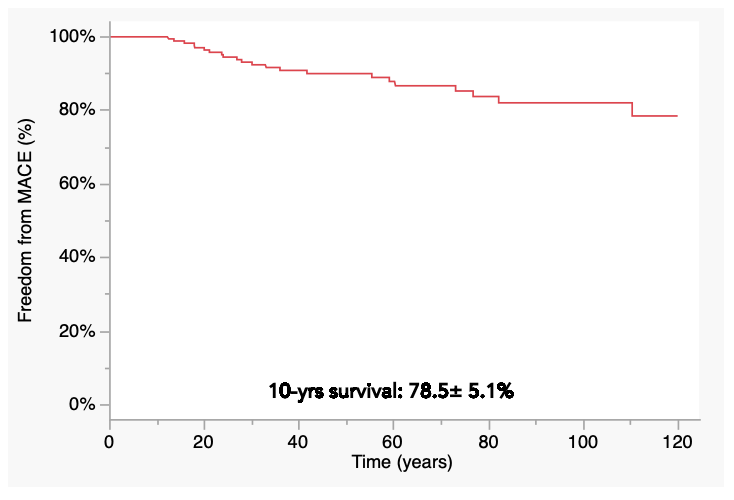
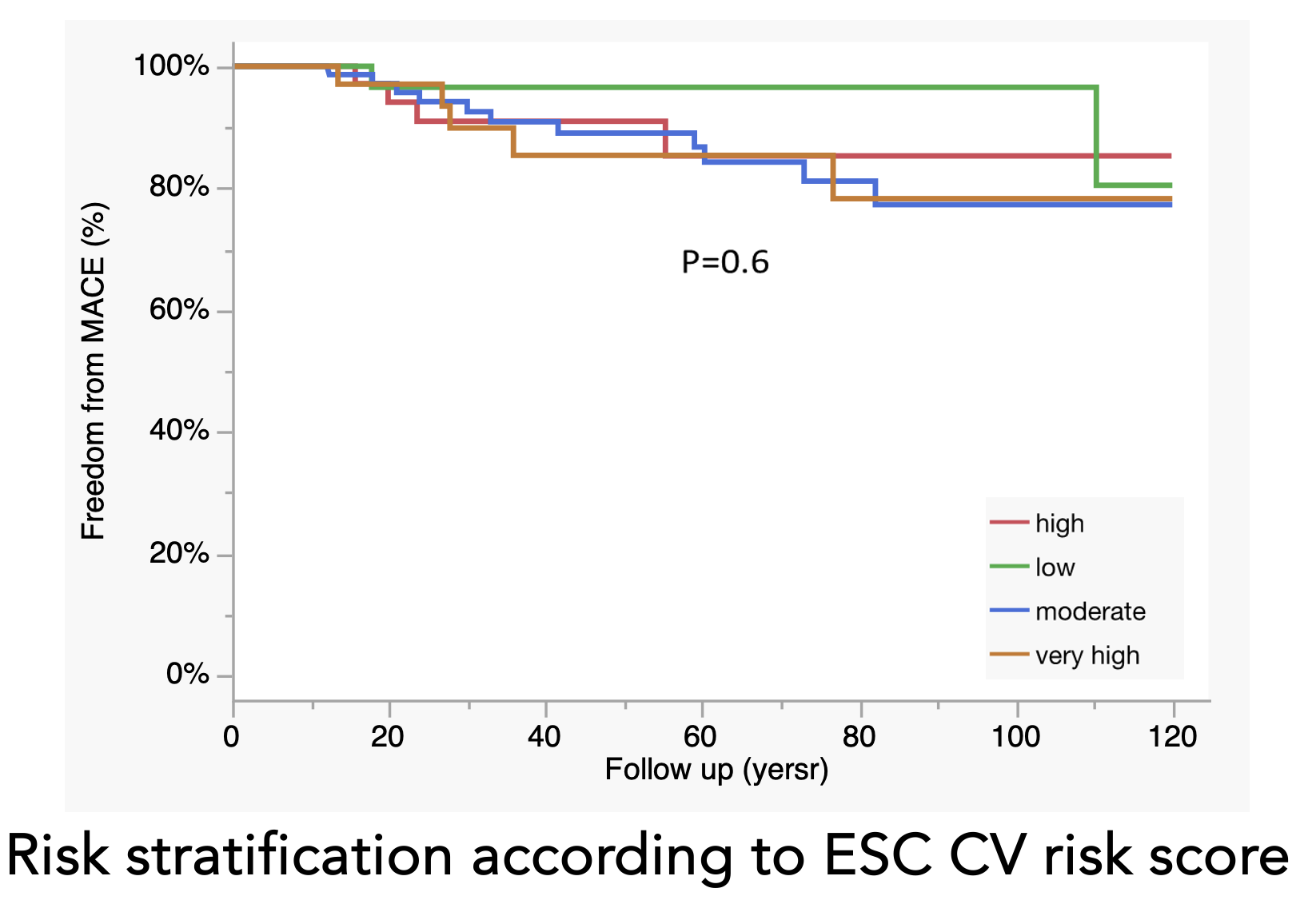
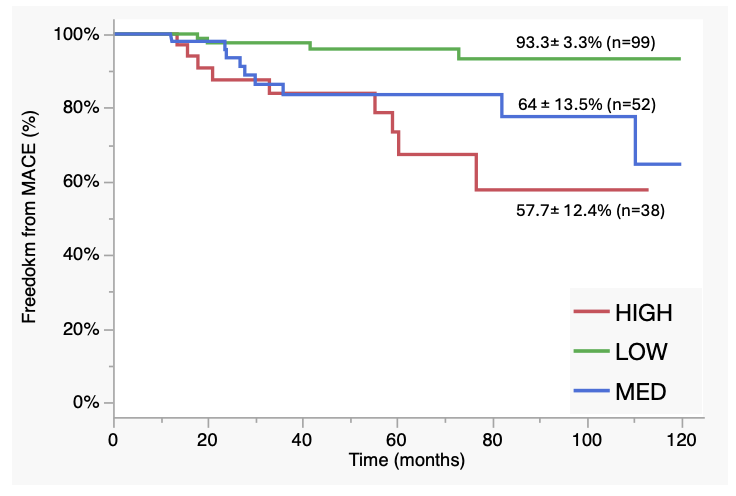
Purpose: recent ISHLT guidelines for heart transplant (HT) recipients recommend the use of statins; however, no specific LDL-C threshold is defined and cardiovascular (CV) risk stratification is typically carried out as in general population. This study aims to evaluate the feasibility of traditional CV risk charts and assess whether a tailored scoring system is needed for HT patients. Methods: in this single-center study of prospectively collected data, we included all adult HT patients at our center (2013–2023) who survived at least one year post-transplant. We analyzed therapy, metabolic and CV risk factors and coronary allograft vasculopathy (CAV) at one month and one year after HT to identify predictors of long-term outcomes. Patients were stratified into low, intermediate, and high/very high risk groups based on current ESC guidelines. The primary endpoint was 10-year MACE-free survival (excluding cellular rejection). Results: among 189 patients (73% male, mean age 52±12 years), 30% had ischemic cardiomyopathy, 22% diabetes and 70% hypertension; mean donor age was 46±14 years. Stratification based on ESC CV risk charts failed to predict 10-year outcomes (MACE-free survival: 80.4±14.9% vs 77.3±6.5% vs 85.2±7.2% vs 77.2±9.2% for low, intermediate, high, and very high risk, respectively, p=0.6). Univariate analysis identified several 1-year predictors: LDL >110 mg/dL, triglycerides >140 mg/dL (both determined via ROC analysis), cellular rejection (≥2 2R episodes) within the first year (p<0.01 for all), and CAD with borderline significance (p=0.08). Statin use increased significantly during the first year (46.4% to 77.9%, p<0.01), leading to a reduction in LDL levels (129±48 vs 109±38 mg/dL); however, 45% of patients still had LDL >110 mg/dL. Diabetes showed a modest association with CAV at 5 years (p=0.07) but not with MACE. Use of mTOR inhibitors, steroids, antiplatelets and donor-specific antibodies (DSAs) were not predictive of MACE. Stratifying patients into three risk groups based on the number of significant risk factors (0–1 vs 2 vs 3–4) improved prediction of 10-year MACE-free survival (93.2±3.4% vs 64.6±13.5% vs 57.5±12.5%, low, medium, and high risk, p<0.01), even after adjustment for donor age >45 years. Conclusion: traditional CV risk factors are not predictive in HT recipients. A tailored risk score incorporating metabolic factors, rejection history, and ischemic etiology provides superior risk stratification, regardless of donor age.