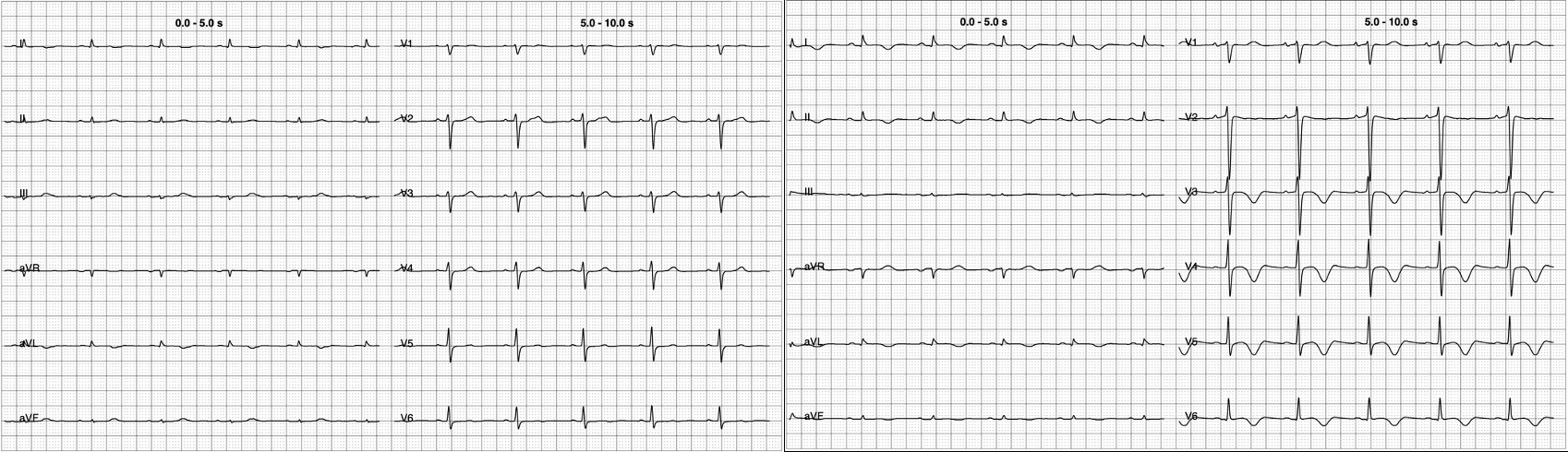
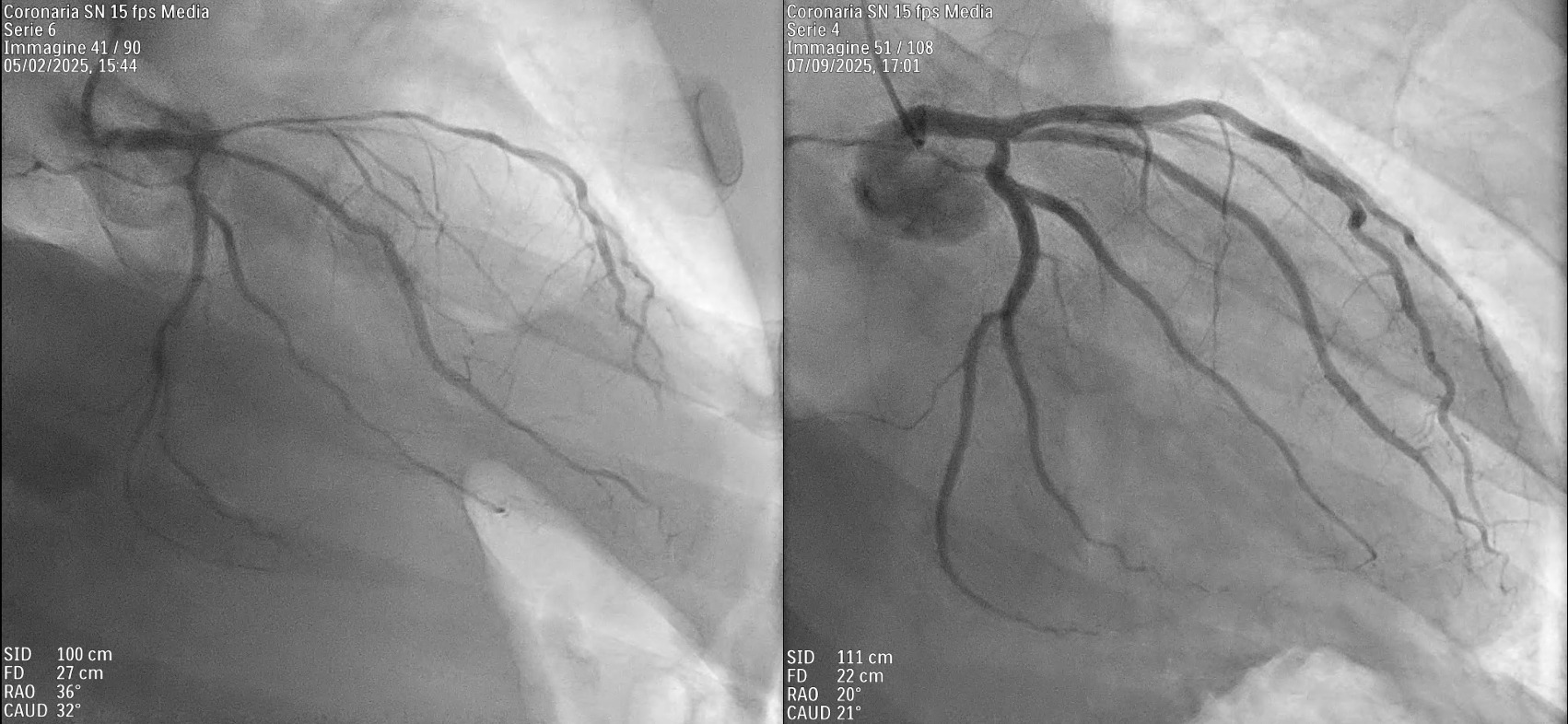
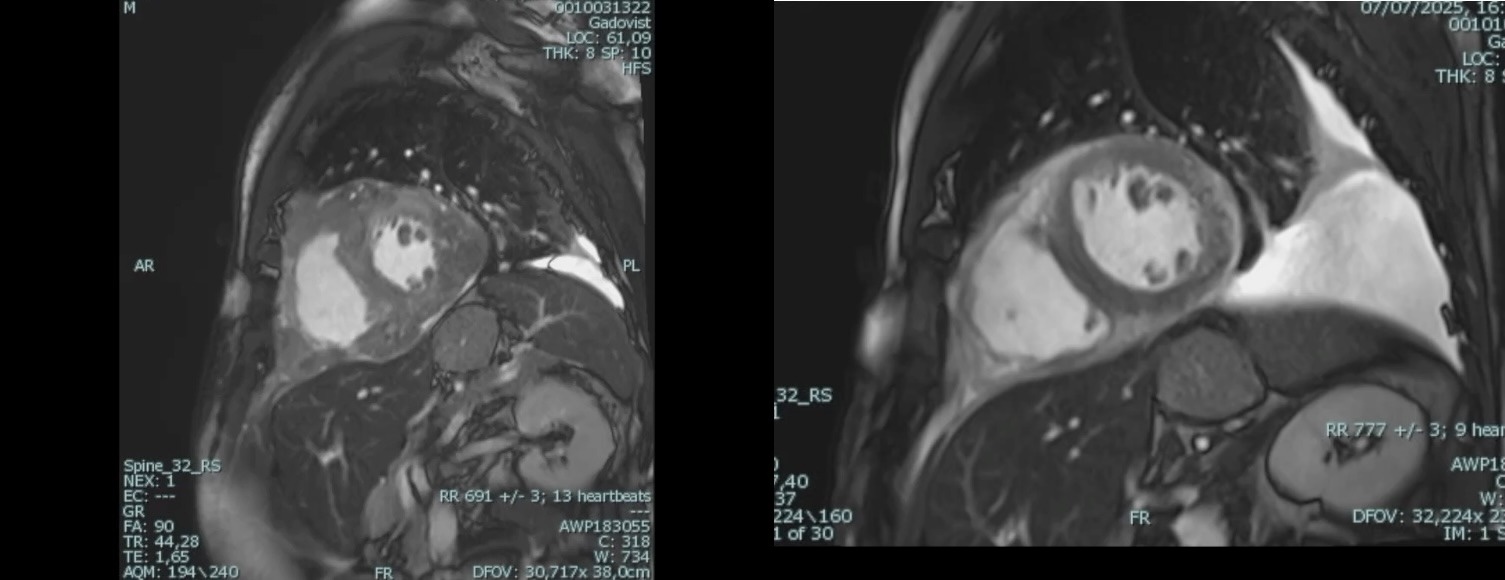
Background Primary cardiac lymphoma is an extremely rare condition, accounting for less than 0.5% of extranodal lymphomas. It can present with a variety of symptoms, including pericardial effusion, heart failure, arrhythmias, or coronary artery compression. Accurate diagnosis requires a multimodal imaging approach—utilizing echocardiography, cardiac magnetic resonance (CMR), and PET-CT—complemented by cytological or histological confirmation. Case Description A 62-year-old male with a history of B-cell lymphoma presented to the Emergency Department with pleuritic chest pain and pericardial and pleural effusions. Despite initial treatment for suspected pericarditis with colchicine and ibuprofen, the patient’s condition progressed to hemodynamic compromise, requiring pericardiocentesis. Cytologic analysis and a supraclavicular mass biopsy confirmed recurrence of high-grade B-cell non-Hodgkin lymphoma. PET-CT imaging showed systemic spread with significant cardiac and pleural uptake. During hospitalization, the patient developed hypoxemia, hypotension, and acute chest pain. CT angiography excluded embolism but identified extrinsic compression of the right pulmonary artery. Concurrently, ECG changes and new regional wall motion abnormalities (posterolateral hypokinesia) appeared, with a decline in left ventricular ejection fraction (LVEF). Coronary angiography demonstrated critical stenoses of the left anterior descending, intermediate, and circumflex arteries, all suggestive of extrinsic compression. CMR further confirmed extensive intramyocardial infiltration. Following the failure of first-line Polatuzumab-Rituximab, second-line therapy with Obinutuzumab and Glofitamab was initiated. This targeted approach led to progressive lesion regression, normalization of ventricular function (LVEF improved from 38% to 56%), and complete resolution of the coronary stenoses. Conclusions This case highlights the importance of considering cardiac lymphoma in the differential diagnosis of recurrent pericardial effusion, unexplained ventricular dysfunction, or atypical coronary stenoses, particularly in patients with a history of lymphoproliferative disease. Integrating advanced imaging with histological confirmation is essential for diagnosis and targeted immunochemotherapy. These therapies can effectively induce mass regression and complete functional cardiac recovery, including the resolution of extrinsic vascular compression.