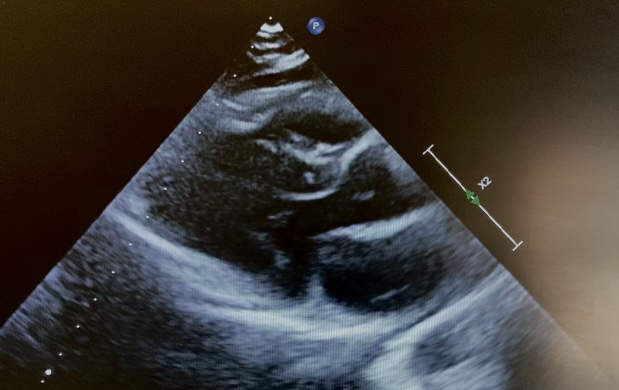
Introduction: Langerhans cell histiocytosis is a rare disease, more common in the pediatric age; the vinblastine–corticosteroid combination represents the first-line treatment. Cardiovascular effects of corticosteroids are generally mild; however, rare cases of obstructive hypertrophic cardiomyopathy have been described, mainly in the neonatal age. We report an exceptional case of reversible obstructive hypertrophic cardiomyopathy in a school-aged child. Clinical case: An 11-year-old boy started treatment for Langerhans cell histiocytosis according to the LCH-IV protocol with vinblastine and prednisone (1 mg/kg/day). After five weeks of therapy, an obstructive hypertrophic cardiomyopathy pattern was incidentally detected: parietal hypertrophy (IVS 10 mm, Z-score +2.8, figure 1) and dynamic left ventricular outflow tract obstruction (max PG 83 mmHg, figure 2) in an asymptomatic child. Over the following 3–4 weeks, during gradual steroid tapering, a complete regression of the condition was observed: echocardiography documented normalization of parietal thickness (IVS 8.5 mm, Z-score +1.1) and absence of outflow tract obstruction. Discussion and conclusions: obstructive hypertrophic cardiomyopathy represents a rare but clinically relevant complication of corticosteroid therapy in pediatric age. Most cases described in the literature involve neonates or infants exposed to high steroid doses, in whom myocardial hypertrophy appears related to the direct anabolic effect of glucocorticoids on the immature myocardium. In school-aged children this event is exceptional and poorly documented, particularly in the context of therapy for Langerhans cell histiocytosis. The reported case is peculiar due to the patient’s age, the absence of symptoms, and the diagnosis made during routine cardiologic surveillance. The close temporal correlation with the initiation of steroid therapy and the rapid and complete regression of the condition after prednisone reduction strongly support a pharmacological etiology. This case highlights the importance of maintaining a high level of clinical awareness and considering targeted cardiologic surveillance in pediatric patients undergoing steroid treatment, especially in cases of prolonged exposure or high doses.