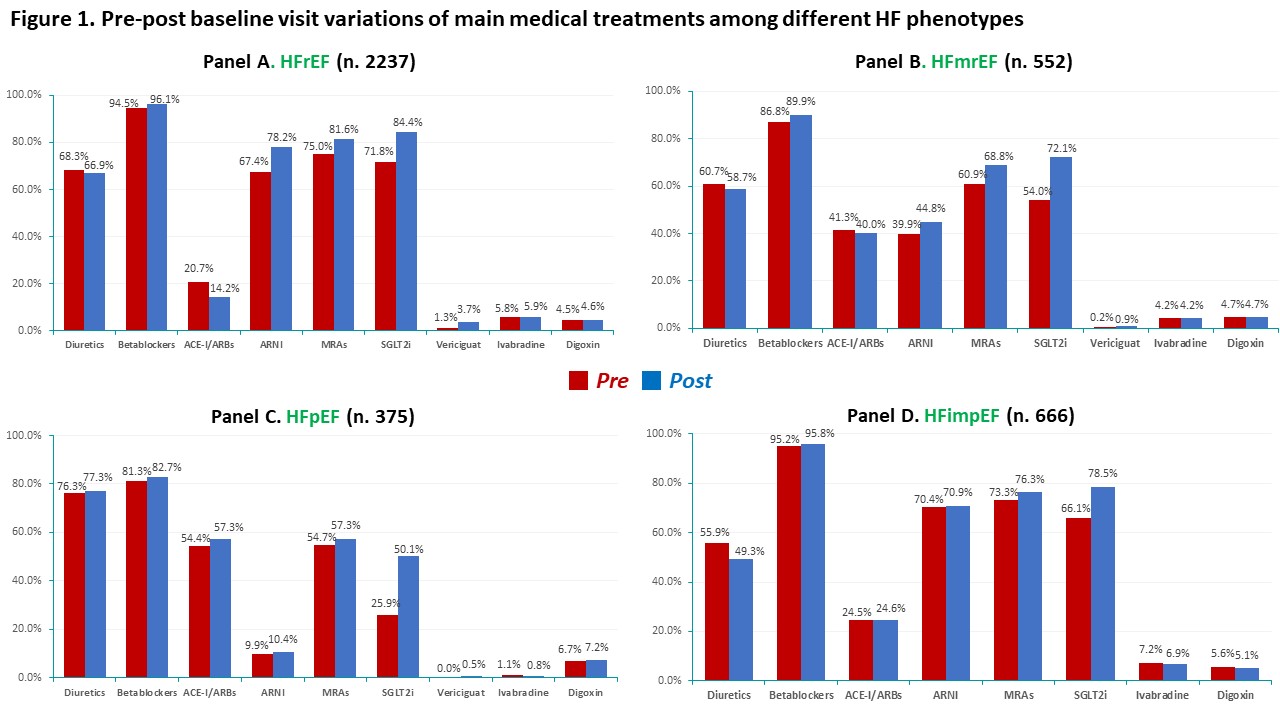
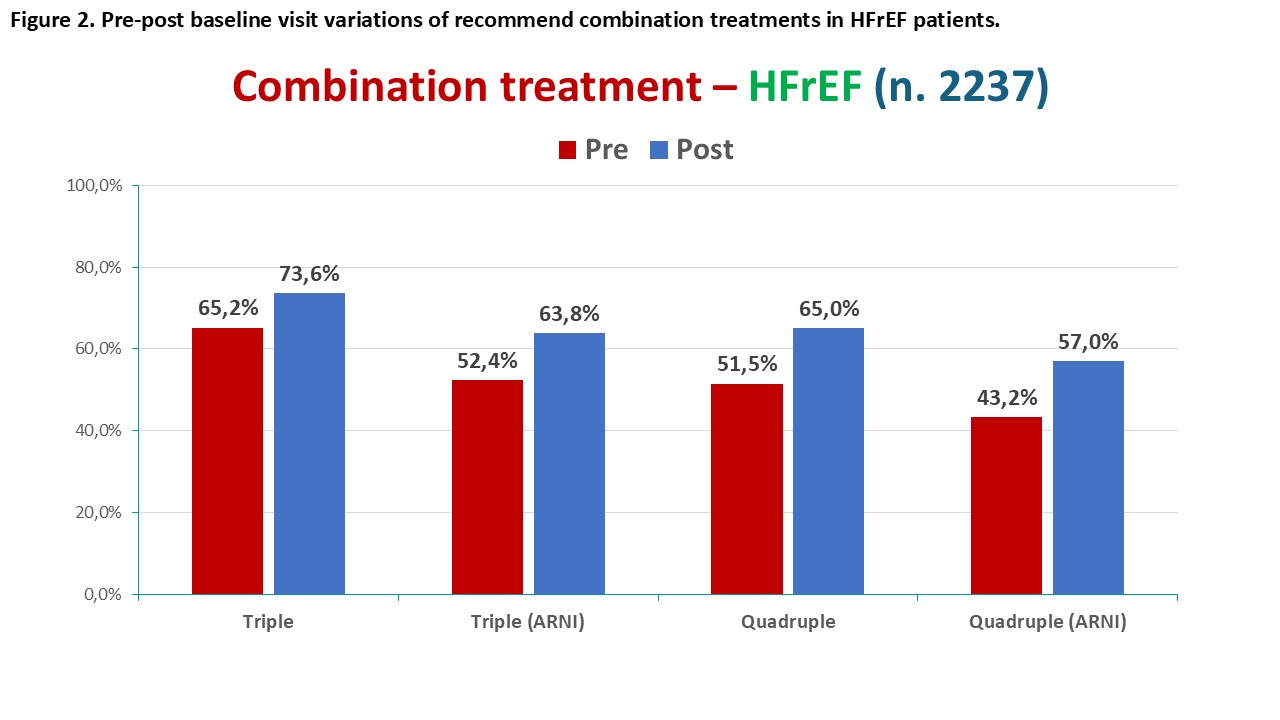
Background: Current ESC guidelines introduced a four-pillar approach for the treatment of HFrEF, and a Class IA recommendation for Empagliflozin and Dapagliflozin in HFmrEF and HFpEF. Objectives: BRING-UP-3 Heart Failure (HF) study was designed to guide the Guideline implementation recommendations in HF patients enrolled by a large sample of Italian cardiology sites. Methods: BRING-UP-3 HF study is an observational, prospective, nationwide investigation encompassing 179 sites enrolling ambulatory and hospitalized HF patients. The study includes an educational intervention followed by two three-month enrollment periods and by a six-month follow-up period with end-point evaluation. For HFrEF patients, the objective is to describe the proportion of patients who receive the four pillars. Here we present the baseline data of the ambulatory cohort. Results: A total of 3,830 ambulatory patients were included in the study. The mean age was 70±12 years (34.5% over 75 years), females were 21.9%. The most prevalent group was HFrEF (58.4%), followed by HFimpEF (17.4%), HFmrEF (14.4%), and HFpEF (9.8%). Hypertension, atrial fibrillation, diabetes mellitus, and chronic kidney disease were reported in 68.2%, 40.4%, 31.0%, and 33.1%, respectively. Figure 1 reports pre-post visit prescription rates of main HF medical treatments among different groups according to ejection fraction phenotypes. beta-blockers and RASi (with ARNIs widely preferred over ACE-I/ARNIs ) were prescribed in over 90% while SGLT2i and MRAs were prescribed in over 80% of cases. Consequently, among HFrEF patients, a high prescription rate of combination treatments could be observed (Figure 2) with 65% of patients being prescribed the four therapeutic pillars. In HFmrEF and HFpEF, SGLT2i prescription rates reached 72.1% and 50.1%, respectively. Conclusions: A comprehensive analysis of a large sample of Italian cardiology sites revealed a high prevalence of prescription of guideline-recommended treatments.