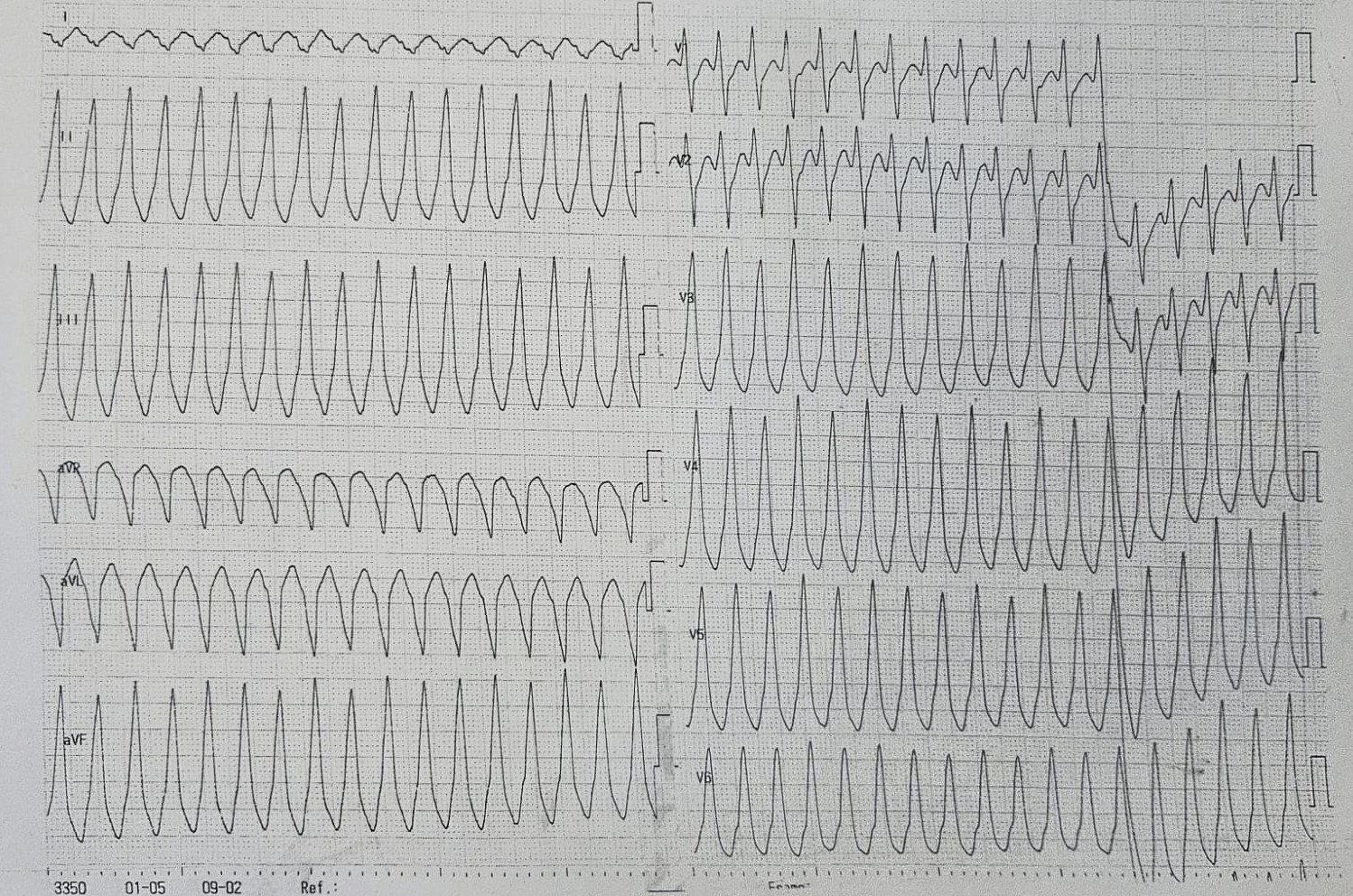
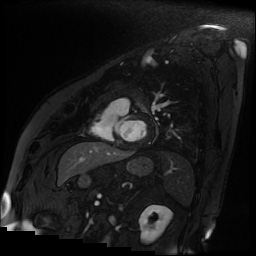
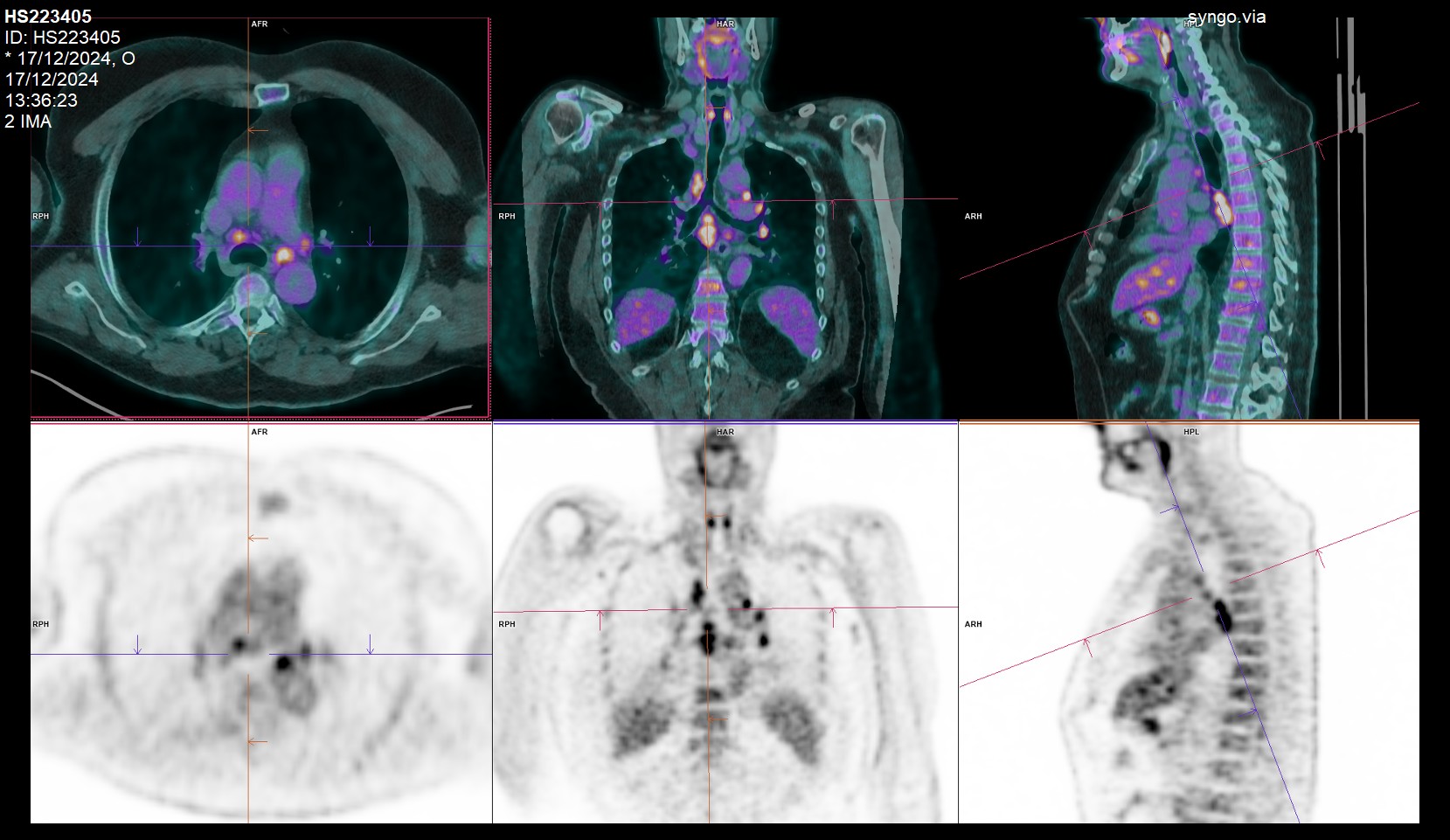
Background: Sarcoidosis is a multisystem inflammatory disease of unknown etiology, commonly affecting the lungs, and lymphatic system. Clinically evident cardiac involvement occurs in about 5% of cases, presenting as bradyarrhythmias, VT, and heart failure. However, many patients have subclinical disease and autopsies show cardiac sarcoidosis (CS) in 20–29% of systemic cases. The true prevalence of CS is underestimated and contributes significantly to morbidity and mortality. Clinical Case: A 56-year-old male with stage I pulmonary sarcoidosis, treated with immunosuppressants, and a family history of sudden cardiac arrest, presented with palpitations and near-syncope. He was hemodynamically stable but had VT at 215 bpm, with a QRS complex positive in V3–V6 and inferior leads, suggesting an LVOT origin. After successful electrical cardioversion (ECV), a TTE revealed apical anterolateral and inferolateral hypokinesis with an EF of 45%. HS-TnI peaked at 432 ng/L post-ECV. Coronary angiography excluded significant stenosis. A cardiac MRI one week later showed hypertrophy of the IVS and normal global contractile function, with no edema on T2-weighted images. LGE was noted in the basal IVS, nearly transmural. T1/T2 mapping and extracellular volume values were elevated in the mid-basal IVS, with FDG-PET positive only in carinal lymph nodes, suggesting systemic involvement and posing a dilemma about using immunosuppression. Based on the HRS 2014 consensus, the patient was diagnosed with probable CS due to histologically confirmed extracardiac sarcoidosis, symptomatic VT, and typical LGE positivity. However, other cardiac causes, such as arrhythmogenic cardiomyopathy, could not be excluded due to limited family history information. Given the clinical presentation and family history, a dual-chamber ICD was implanted for secondary prevention, in line with 2022 ACC/AHA/HRS guidelines. Absent edema on CMR and negative cardiac FDG-PET ruled out active inflammation, but a myocardial scar was identified, likely the arrhythmogenic focus. Thus immunosuppressive therapy was not initiated and we started amiodarone as antiarrhythmic therapy. Although histologic confirmation of CS is not mandatory, it may aid prognosis stratification. If VT recurs with ICD discharges, catheter-based RFA may be considered to reduce mortality and prevent heart failure progression. Conclusion: Immunosuppressants are effective for inflammation but not scar-related VT and should be used selectively