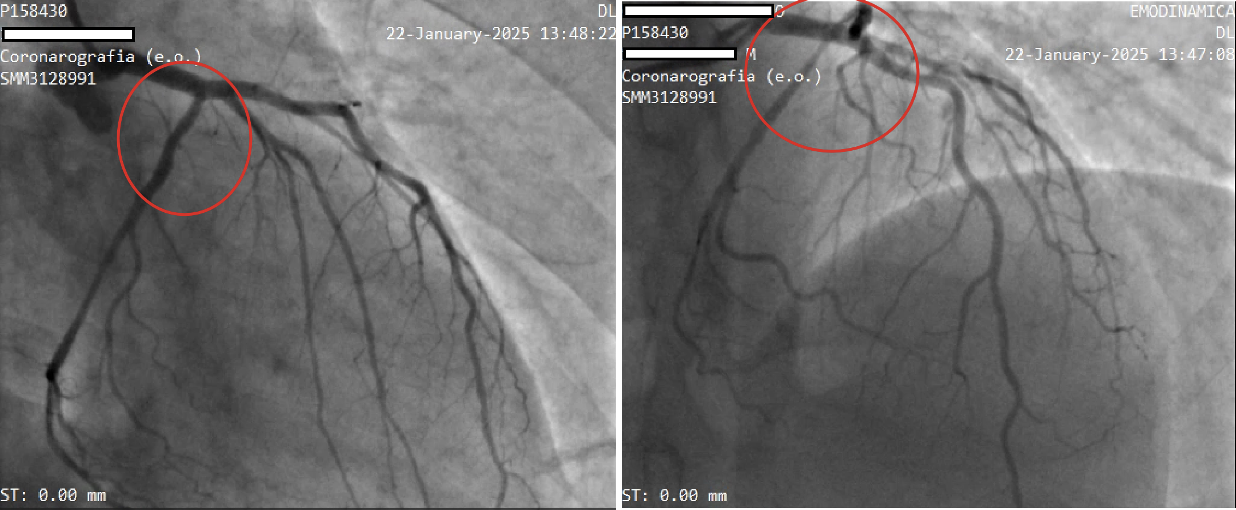
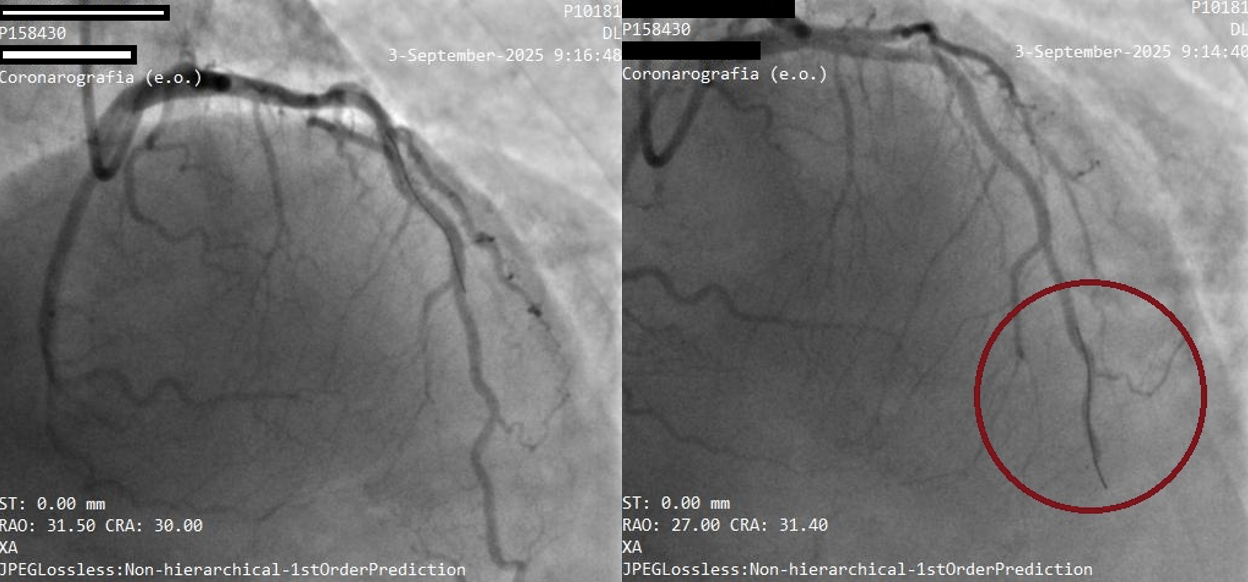
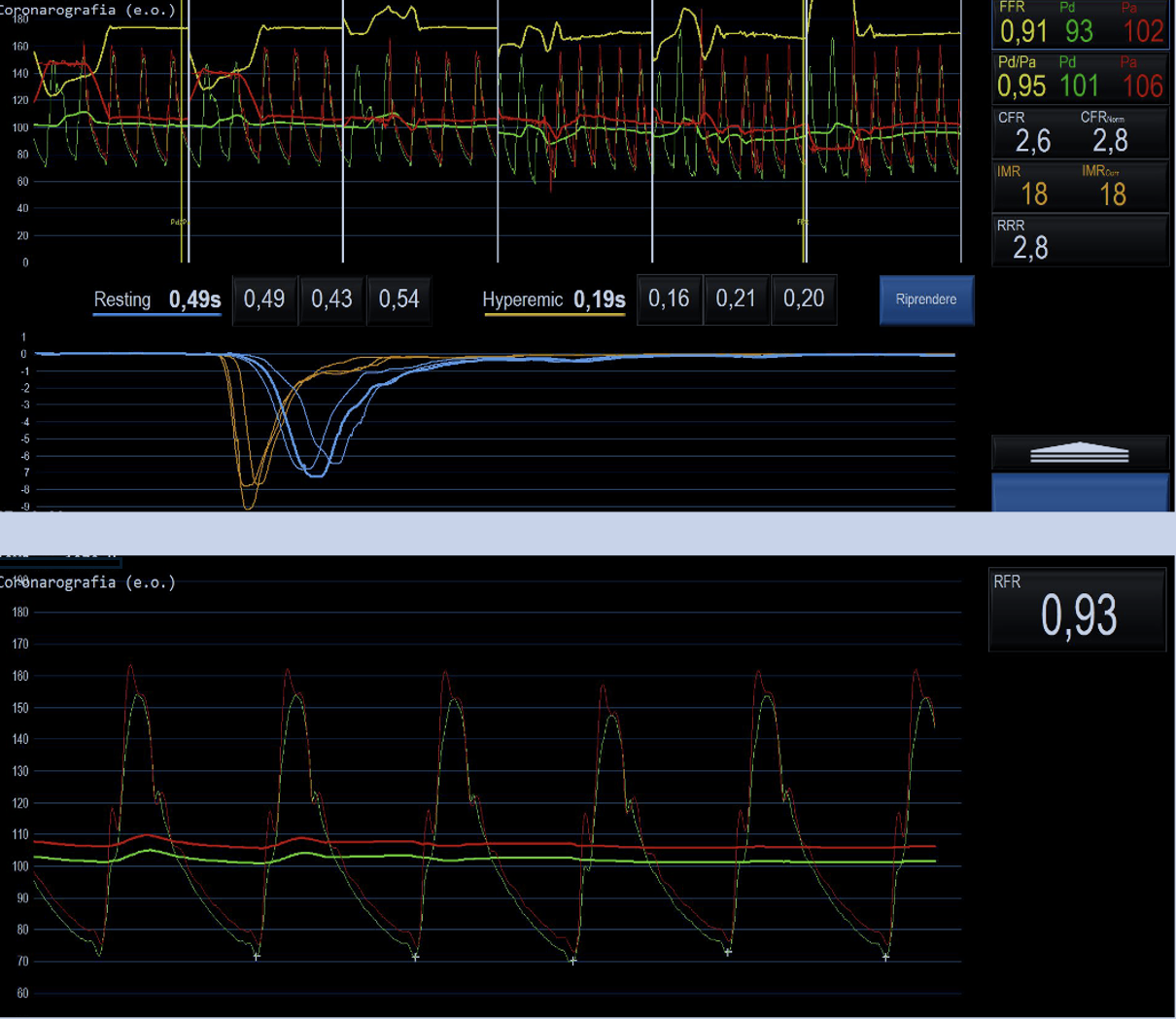
Introduction Coronary vasospasm is a recognized cause of MINOCA and usually responds to calcium-channel blockers and nitrates. A minority of patients develops severe refractory vasospastic angina with recurrent ischemia. Case Report A 55-year-old man presented with resting chest pain and elevated high-sensitivity troponin. Coronary angiography showed non-critical coronary atherosclerosis; cardiac MRI revealed transient edema. A diagnosis of vasospastic MINOCA was suspected and amlodipine initiated. Recurrent episodes in July and October 2024 prompted acetylcholine testing, positive at 50 µg for epicardial vasospasm, with preserved microvascular function. Therapy was progressively intensified (diltiazem, nitrates, dihydropyridine CCBs, ranolazine) with smoking cessation. In January 2025 he developed a new ischemic event complicated by complete atrioventricular block due to circumflex artery spasm (Fig.1). Given rapid progression and refractoriness to maximal therapy, cardiac sympathetic denervation was performed in “Molinette” Hospital in Turin. At follow-up in September 2025, full physiological assessment confirmed normal microvascular indices (Fig.3). Acetylcholine testing remained positive at 50 µg but the patient remained completely free of anginal or ischemic events (Fig.2). Discussion Vasospasm arises from smooth muscle hyperreactivity, endothelial dysfunction and autonomic imbalance. Excessive sympathetic activation may sustain vasomotor instability through stellate ganglion remodeling and cardio-spinal reflex pathways. Sympathetic denervation interrupts these circuits, representing a valuable option in selected refractory cases, as demonstrated in this patient. Conclusion This case highlights an exceptional form of coronary vasospasm unresponsive to all available therapies and complicated by recurrent MINOCA and conduction disturbances. Cardiac sympathetic denervation resulted in marked clinical stabilization despite persistent angiographic vasoreactivity. In view of the complete absence of further ischemic episodes, no additional interventions were pursued, and the patient remains under clinical and angiographic follow-up. Future perspectives may include regenerative strategies such as autologous CD34+ stem cell therapy, a promising approach for endothelial and microvascular dysfunction that warrants dedicated investigation.