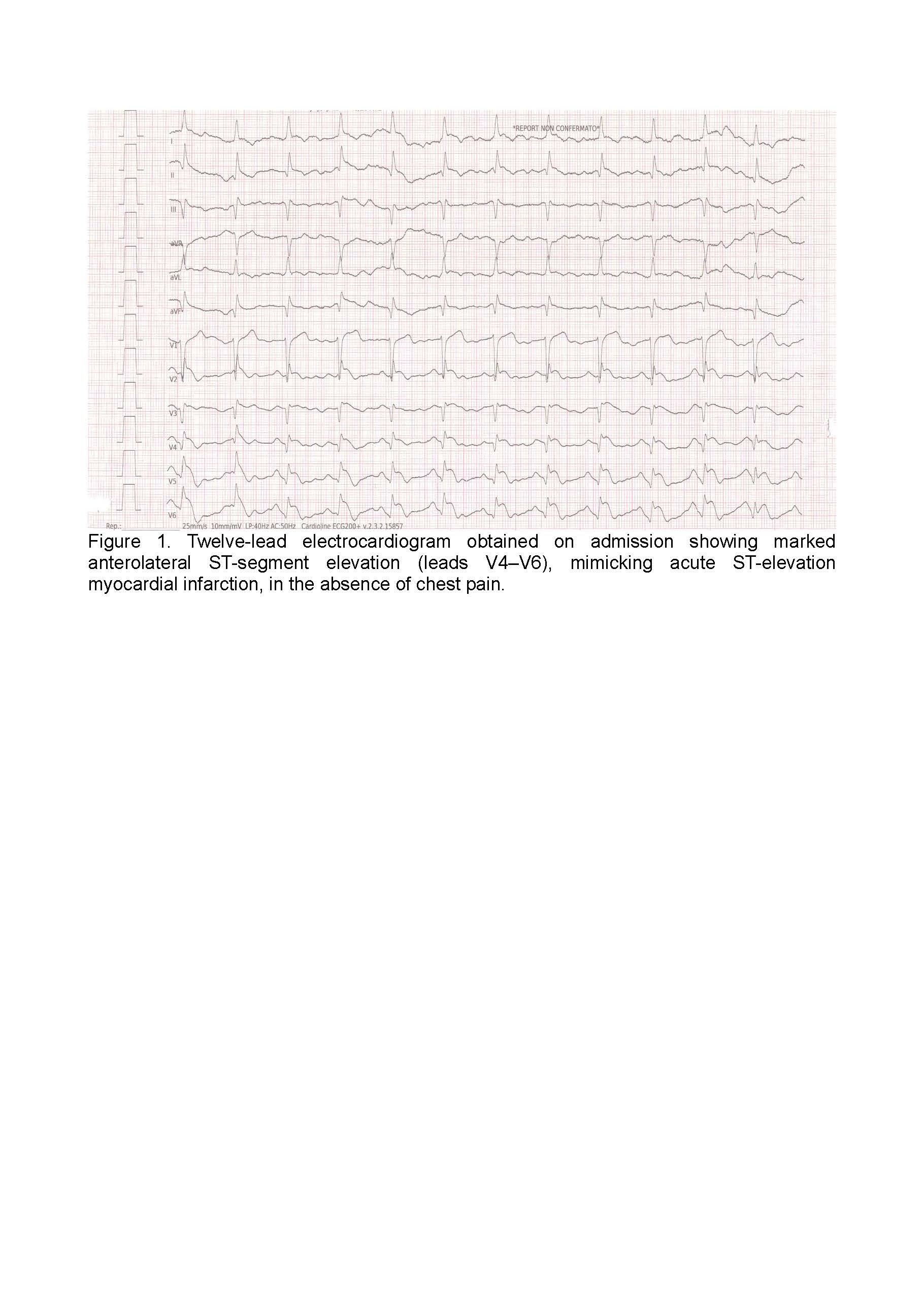
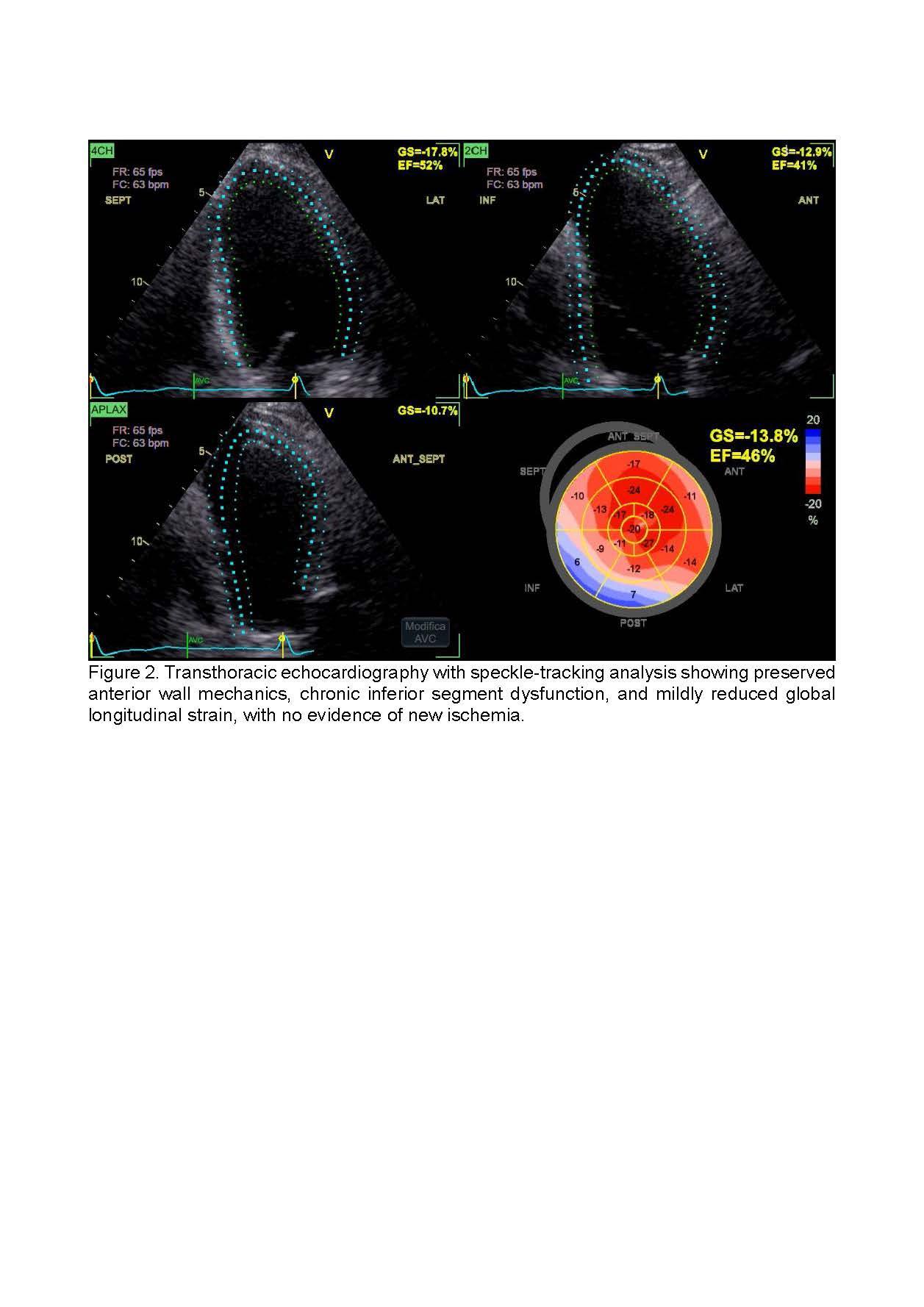
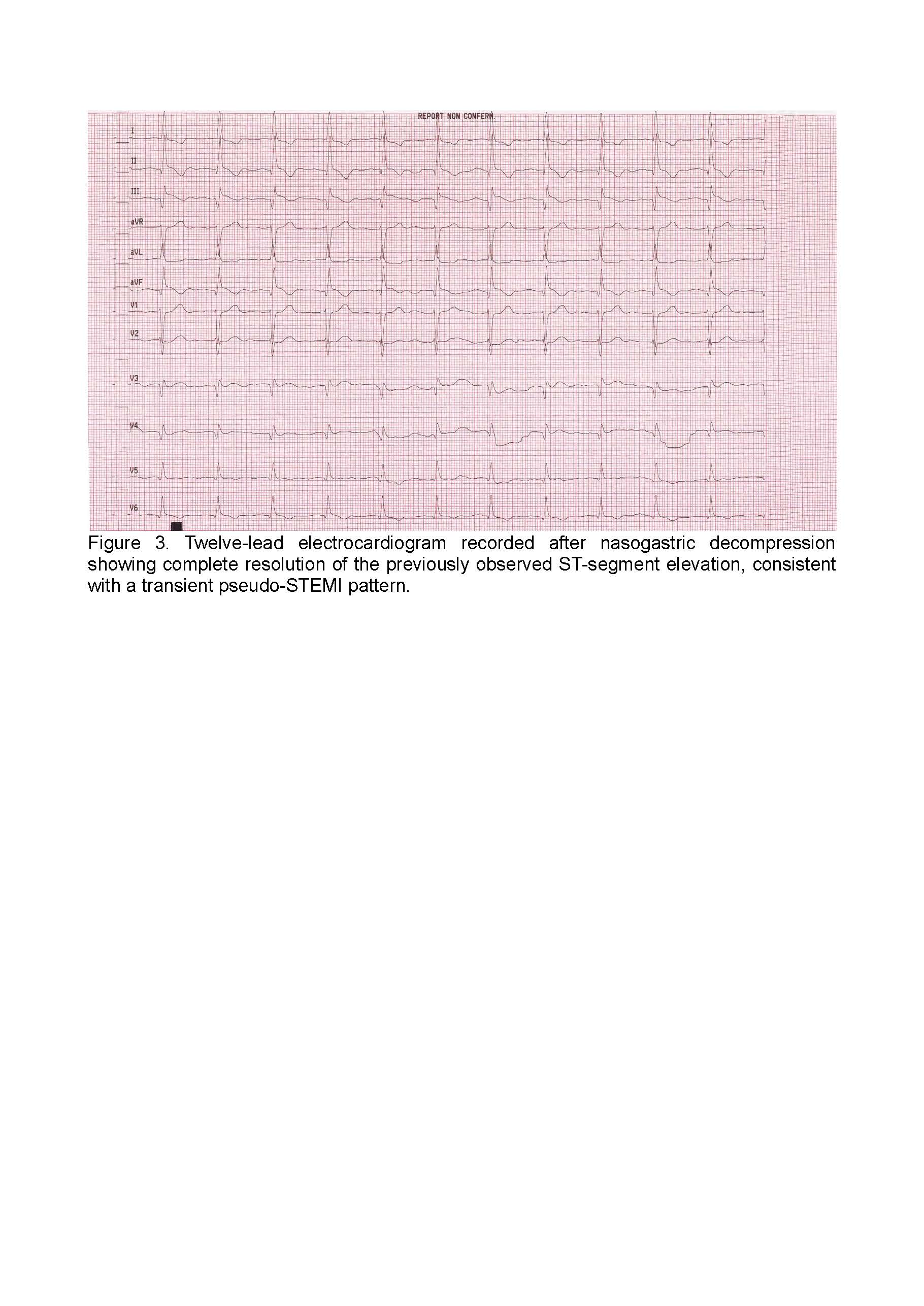
Background: ST-segment elevation on electrocardiography is commonly interpreted as a marker of acute coronary artery occlusion. However, extracardiac conditions may occasionally produce pseudo-ischemic electrocardiographic patterns, posing significant diagnostic challenges and increasing the risk of unnecessary invasive procedures. Case presentation: We report the case of a 68-year-old man with a history of inferior myocardial infarction who presented to the emergency department with severe abdominal distension due to a closed-loop small bowel obstruction. Despite the absence of chest pain or cardiopulmonary symptoms, the admission electrocardiogram showed marked anterolateral ST-segment elevation fulfilling diagnostic criteria for ST-elevation myocardial infarction. High-sensitivity troponin levels were negative. Prompt transthoracic echocardiography demonstrated preserved anterior wall motion, chronic inferior akinesia consistent with prior infarction, and unchanged global longitudinal strain, effectively excluding acute myocardial ischemia. Nasogastric decompression led to rapid resolution of abdominal distension and complete normalization of ST-segment elevation within fifteen minutes. Subsequent abdominal imaging confirmed a closed-loop volvulus requiring urgent surgical intervention, with full bowel viability preserved after adhesiolysis. Conclusions: This case highlights severe gastrointestinal distension as a rare but clinically relevant cause of transient ST-segment elevation mimicking acute myocardial infarction. Integration of clinical presentation, cardiac biomarkers, and rapid echocardiographic assessment, including strain imaging, is crucial to distinguish pseudo-STEMI from true ischemic events. Recognizing extracardiac causes of ST-segment elevation may prevent unnecessary coronary angiography while ensuring timely management of underlying surgical emergencies.