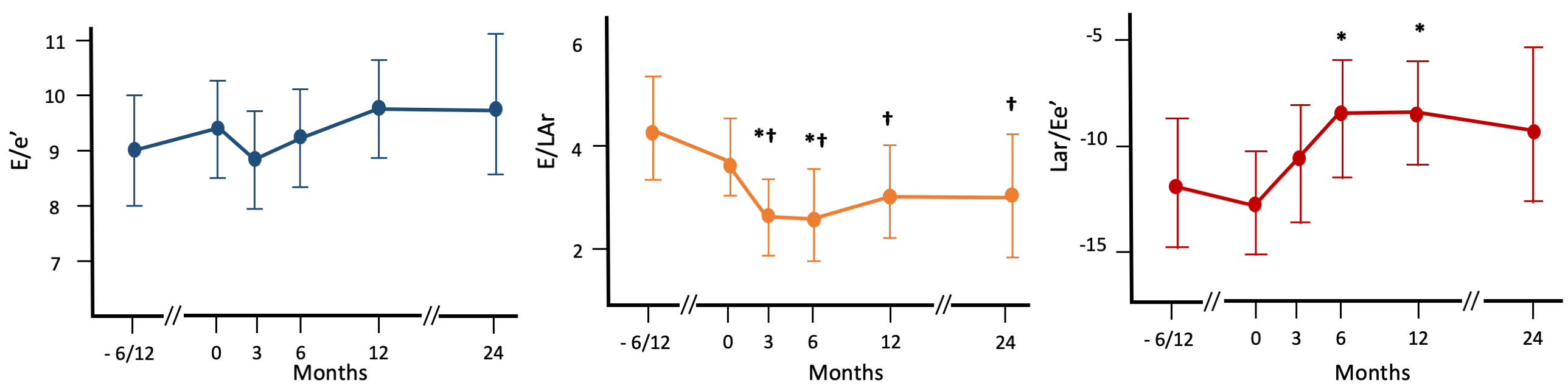
Background. The type 2 sodium-glucose cotransporter inhibitors (SGLT2i) are milestone drugs in the treatment of heart failure with reduced ejection fraction (HFrEF). However, the mechanisms responsible for their beneficial effects are still to be clarified. Aim of the study. To evaluate the effect of SGLT2i therapy on left ventricular filling pressure in a group of HFrEF outpatients by analysing changes in traditional and new echocardiographic parameters. Methods. Before and 3, 6, 12, and 24 months after the introduction of SGLT2i, the following traditional and new echocardiographic indices reflecting left ventricular filling pressures were evaluated: – the ratio between early diastolic peak at pulsed Doppler (E) and the mean septal-lateral mitral early diastolic peak at TDI (E/e’); – the maximal deformation of the left atrium (left atrial reservoir, LAr) by two-dimensional speckle tracking analysis; – the ratio between E and LAr (E/LAr); – the ratio between LAr and E/e’ (LAr/Ee’). In a subgroup of patients, an echocardiographic evaluation was performed 6-12 months before SGLT2i introduction. Changes in the repeated measures were evaluated by linear mixed models. A p<0.05 was considered significant. Results. We enrolled 60 HFrEF outpatients (83% males, age 61 ± 13, mean LVEF 31 ± 7%, NYHA class II in 75% and III in 25%), all in conventional medical therapy (sacubitril/valsartan or ACE- inhibitors or angiotensin II receptor blockers in 100%, beta-blockers in 100%, mineralcorticoid receptor antagonists in 87%, loop diuretics in 62%). As shown in the Figure, E/e’ did not significantly change during follow-up. In contrast, the E/LAr ratio significantly decreased from 3 months onward, while LAr/e’ increased significantly over the same time period. Conclusions. These findings indicate that SGLT2 inhibitors can reduce left ventricular filling pressure evaluated by new derived echocardiographic indices in HFrEF patients already receiving optimised medical therapy. These findings highlight the potential role of SGLT2i in improving diastolic function and atrial-ventricular coupling in HFrEF.