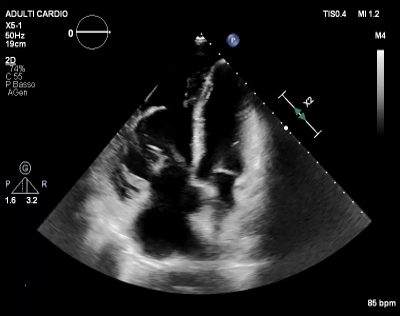
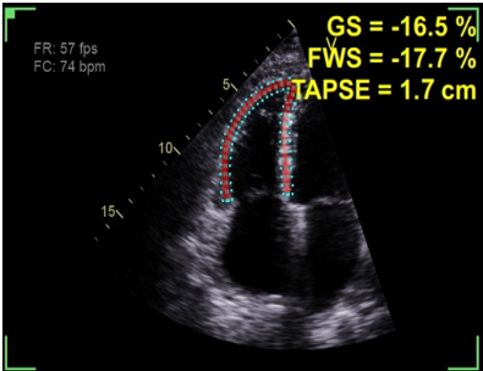
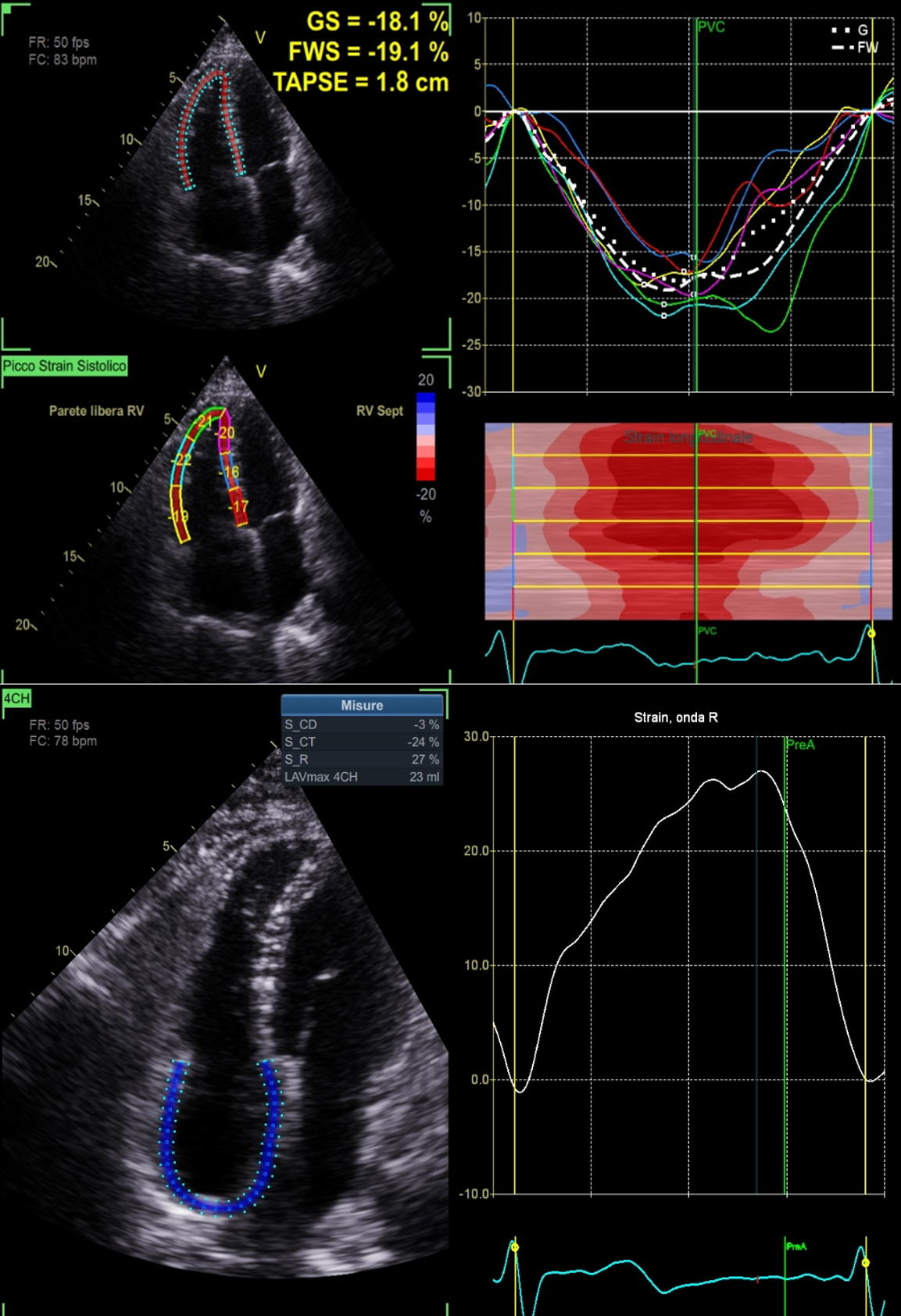
Risk stratification in pulmonary arterial hypertension (PAH) is critical for prognosis and treatment decisions, yet current models—including ESC/ERS tables, REVEAL, and COMPERA—have significant limitations. They inadequately account for dynamic right–ventricular (RV) function, genetic factors, and individual comorbidities. Approximately 40% of patients classified as low risk deteriorate despite guideline–based therapy, indicating that risk assessment may be incomplete and may lead to suboptimal treatment choices. Traditional noninvasive markers, such as WHO functional class, 6–minute walk distance, and BNP/NT–proBNP, are subjective and non specific. Echocardiography is increasingly recognized as a key tool for early detection of RV dysfunction and monitoring therapy. TAPSE <18 mm, RV/RA dilation, and RV end–systolic remodeling correlate with worse outcomes, but individual measures may not capture load–dependent RV–pulmonary arterial interactions. The TAPSE/PASP ratio, reflecting RV–PA coupling, appears superior, providing a more comprehensive assessment of RV function under pulmonary load. Sotatercept, a TGF–β/activin pathway modulator, has shown significant reductions in pulmonary vascular resistance, improved functional capacity, and decreased composite cardiovascular risk in high–risk patients on maximal therapy, highlighting the need for updated risk thresholds and personalized treatment strategies. A clinical case illustrates these principles: a 40–year–old man presented with dyspnea, leg edema, elevated NT–proBNP, right ventricular strain on ECG, and CT evidence of pulmonary artery and right heart dilation. Echocardiography revealed severe RV dilation, hypokinesia, tricuspid regurgitation, high PASP, and impaired RV–PA coupling. Despite improvement to intermediate–low risk on standard criteria after triple therapy, advanded echocardiogrphy revealed persistent subtle RV dysfunction (reduced TAPSE/SPAP and impaired RVFWS) despite normalized conventional parameters, prompting the addition of sotatercept. After one year, the patient achieved NYHA class I, normalized pulmonary resistance, and complete echocardiographic remodeling. This case emphasizes the limitations of static risk tables and the importance of integrating advanced echocardiographic markers into risk assessment. Sotatercept demonstrates the potential for a new era of therapy, where non invasive dynamic monitoring of RV function can guide treatment optimization and improve outcomes in PAH.