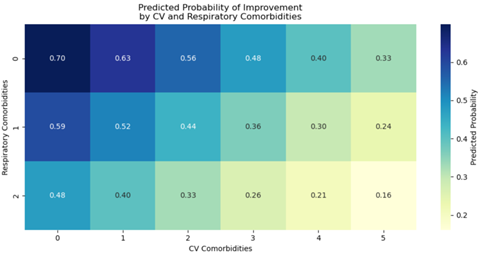
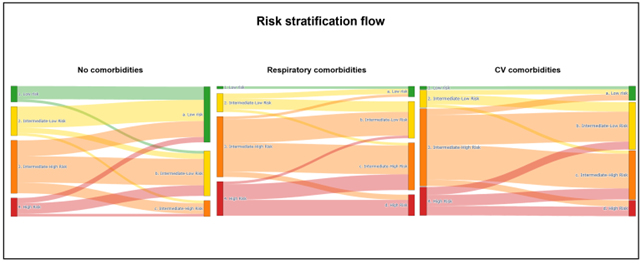
Background: An increasing number of older patients are currently being diagnosed with idiopathic pulmonary arterial hypertension (iPAH) and heritable PAH (HPAH). In this population, cardiovascular (CVc) or respiratory (Rc) comorbidities are common and can affect response to PAH therapies, hence clinical guidelines advise a cautious approach to treatment. The prognostic impact of CVc and Rc in this population remains uncertain. Method and Aims: We retrospectively analysed iPAH and HPAH patients with and without comorbidities and assessed the influence of CVc and Rc on the likelihood of clinical improvement after initiation of PAH therapies by at least one ERS/ESC risk class (four-strata model), as defined by BNP levels, WHO functional class (WHO-FC), and 6MWD. We collected data on 13 comorbidities. ERS/ESC risk scores were assessed at baseline (T0) and T1 (within 3-12 months). Results: A total of 135 patients with iPAH or HPAH were included, 91 with and 44 without comorbidities. Mean age was 60 years old and was higher in patients with comorbidities (p=0.0009). The probability of clinical improvement by at least one risk class was 70.5% ( p = 0.02). An increasing number of CVc and Rc progressively reduced the probability of improvement: each additional CVc significantly reduced the odds of improvement by 27% ( p = 0.018), while each additional Rc was associated with lower odds of improvement (OR = 0.62, p = 0.168). Therefore, though statistical significance was not reached, there appeared to be a greater negative effect in patients with Rc. If only 1 CVc is present, the probability of improvement is equal to patients without comorbidities (χ 2 =1.94, p = 0.16), supporting optimized treatment in this group. Conclusions: Compared to CVc, Rc appear to have a stronger negative impact on treatment response in patients with iPAH and HPAH. Although CVc also negatively affect the probability of improvement, patients with a single CVc show a response similar to the control group, supporting the benefit of optimized therapy in this subgroup. Figure 1: heatmap from a binary multivariable logistic regression illustrating the predicted probability of clinical improvement according to the number of cardiovascular and respiratory comorbidities. Figure 2: changes in risk classification from T0 to T1 according to the ESC/ERS four-strata model in patients without comorbidities (left), with respiratory comorbidities (middle), and with cardiovascular comorbidities (right).