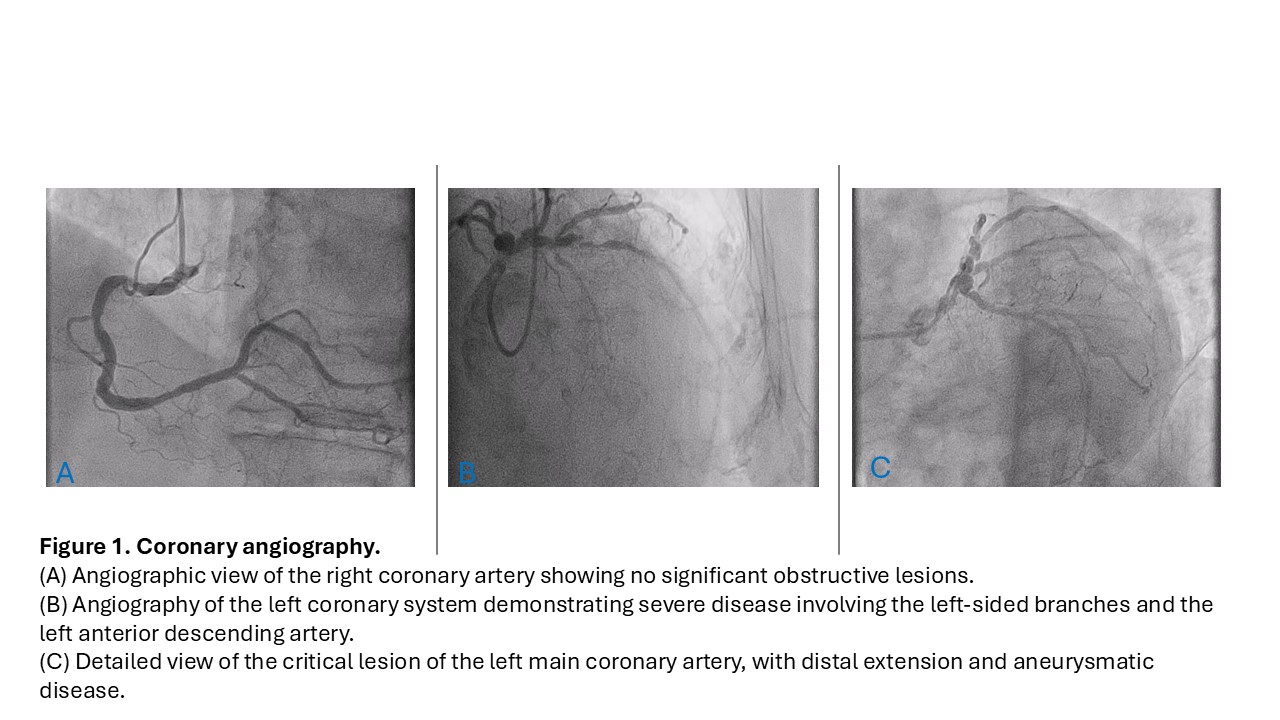
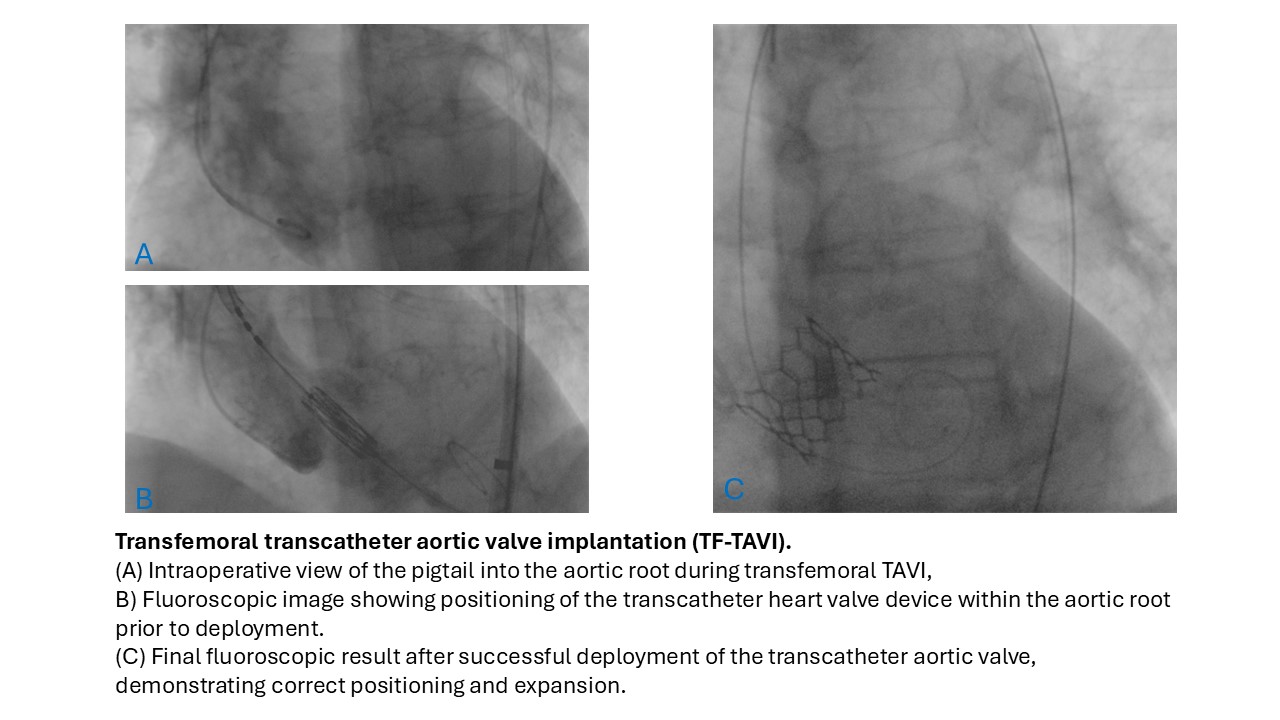
Background Severe aortic stenosis (AS) and coronary artery disease (CAD) commonly coexist in elderly patients and pose a therapeutic challenge, particularly in the presence of frailty and high surgical risk. Conventional surgical approach may be associated with prohibitive perioperative risk, whereas a fully percutaneous strategy may be limited by complex coronary anatomy. Hybrid approaches integrating minimally invasive surgical and transcatheter techniques may represent an alternative in selected patients. Case Summary An 85-year-old man presented with symptomatic severe AS (NHYA class III) and complex CAD. Echocardiography showed severe aortic valve stenosis (area 0.7 cm²; indexed 0.39 cm²/m²; mean gradient 56 mmHg) with preserved left ventricular ejection fraction. Coronary angiography revealed critical distal left main disease with aneurysmatic involvement extending to the origin of the left anterior descending (LAD) artery; left circumflex artery was a small vessel supplying limited area. Surgical risk was elevated (EuroSCORE II 6.87%, STS score 6.54%). After Heart Team discussion, a hybrid strategy was chosen. MIDCAB was preferred over percutaneous coronary intervention due to extensive calcification and unfavorable coronary anatomy, while AS was treated with a transfemoral transcatheter approach to avoid cardiopulmonary bypass. MIDCAB was performed via left anterior mini-thoracotomy with off-pump left internal mammary artery–LAD anastomosis. During the same session, TF-TAVI was successfully performed using a 26-mm Edwards Sapien 3 Ultra™ valve. The procedure was completed in a hybrid operating room by a single cardiac surgical team, with on-table extubation according to an ERAS protocol. The postoperative course was uncomplicated except for transient new-onset atrial fibrillation. At discharge and at 12-month follow-up, echocardiography confirmed optimal valve performance, and the patient was in NYHA class II without angina. Discussion and Conclusion This case demonstrates the feasibility of an hybrid approach combining MIDCAB and TF-TAVI in a selected elderly, high-risk patient with severe AS and complex CAD. The strategy allowed effective treatment of the most prognostically relevant lesions while minimizing surgical trauma and avoiding cardiopulmonary bypass. Careful patient selection, multidisciplinary Heart Team evaluation, and performance in a specialized center were essential for a favorable outcome.