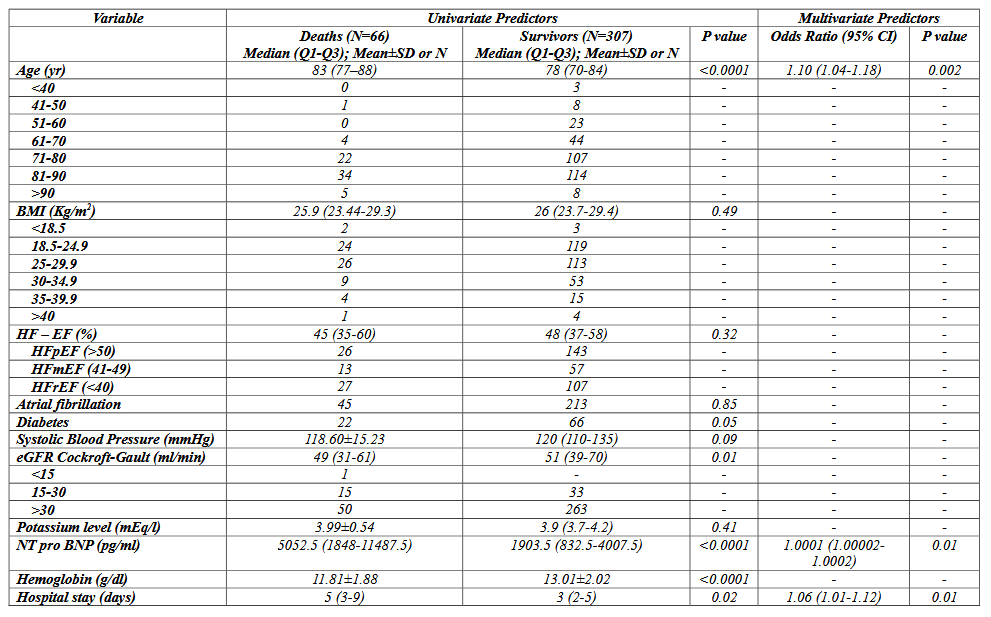
Introduction Acute decompensated heart failure (ADHF) remains a leading cause of hospitalization and mortality worldwide despite therapeutic advances. Early identification of patients at increased risk of adverse outcomes is crucial to improve clinical decision-making and optimize management strategies. Although early and accelerated treatment approaches may enhance hemodynamic stabilization, their impact on mortality and prognostic determinants in ADHF remains incompletely defined. Purpose This study aimed to identify predictors of mortality in patients hospitalized for ADHF and treated with an early and accelerated therapeutic strategy, with particular focus on the four foundational pillars of heart failure therapy. Methods We retrospectively analyzed 373 consecutive patients admitted with ADHF from the Emergency Department to our Cardiology Unit between August 2023 and December 2024. All-cause mortality at 1 year was assessed using ongoing registries and clinical studies conducted in our centre. Univariate and multivariate analyses were performed to identify independent predictors of mortality. Results The mean age was 76.5 ± 10.8 years, and 59.5% of patients were male. Mean body mass index was 26.8 ± 4.7, and 23.6% had diabetes mellitus. Heart failure phenotypes included HFrEF in 27.6%, HFmrEF in 26.8%, and HFpEF in 45.6%. Atrial fibrillation was present in 69% of patients. At discharge, 18.2% had an implantable cardioverter-defibrillator and 2.7% a wearable cardioverter-defibrillator. The 1-year all-cause mortality rate was 17.6%. On univariate analysis, mortality was significantly associated with age, diabetes, eGFR <30 mL/min, anemia, NT-proBNP levels, and length of hospital stay. Multivariate analysis identified age (OR 1.10; 95% CI 1.04–1.18; p=0.002) and length of hospital stay (OR 1.06; 95% CI 1.01–1.12; p=0.02) as independent predictors of mortality. Discussion In this real-world cohort, 1-year mortality remained substantial despite early and accelerated management strategies. Advanced age emerged as the strongest independent predictor, reflecting the impact of frailty and comorbidities. Prolonged hospitalization also independently predicted mortality, serving as a marker of disease severity and clinical complexity. These findings highlight the persistent vulnerability of ADHF patients and underscore the importance of early risk stratification, managing comorbidities and optimized in-hospital treatment, even within accelerated pathways.