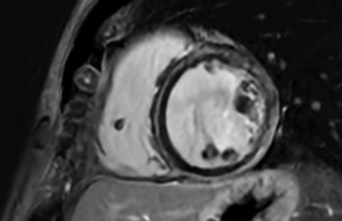
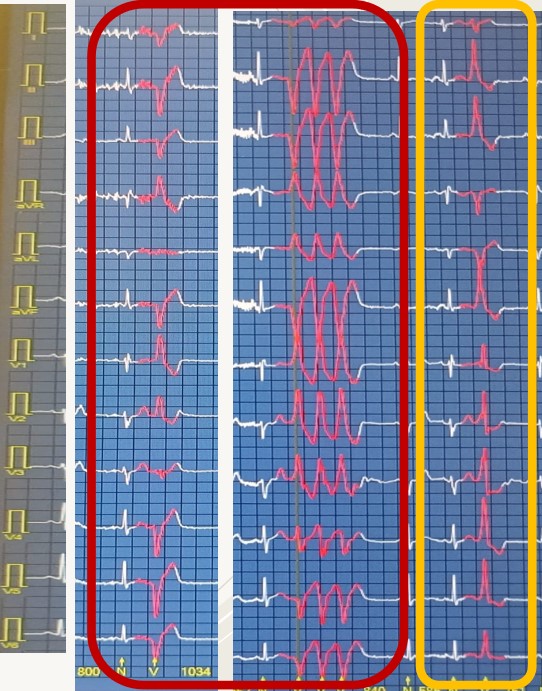
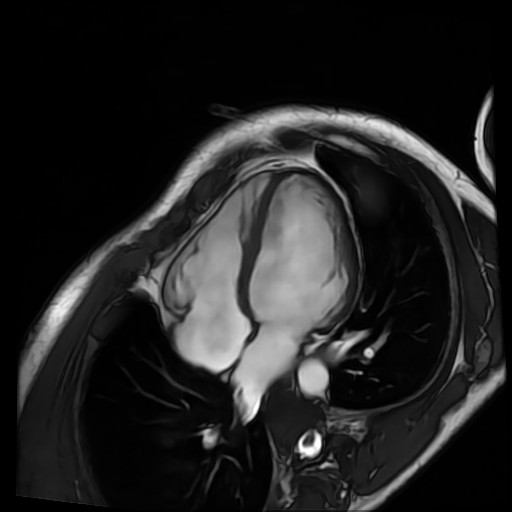
A 31-year-old man, smoker and asthmatic on inhaled therapy, his first-degree uncle has an ICD for secondary prevention following syncope due to sustained ventricular tachycardia (cardiac MRI suggested previous myocarditis). He undergoes a cardiology examination because he has been complaining of dyspnea and extrasystolic palpitations for two years, along with three episodes of presyncope, not predominantly exercise-induced symptoms. The patient is in good hemodynamic compensation, blood tests are normal. The ECG shows isolated ventricular ectopic beats and low voltages in the peripheral leads. The echocardiogram shows a mildly dilated left ventricle (80 ml/m2), mild left ventricular systolic dysfunction (biplane EF 45%) due to diffuse hypokinesia. The Holter ECG shows a high ventricular ectopic burden (3%), several couples and triplets of ventricular ectopic beats, and a brief burst of non-sustained ventricular tachycardia; the morphology of the ectopic beats (right bundle branch block) suggests a left ventricular origin. An exercise test was performed, revealing apparently benign behavior of the BEVs due to their disappearance at peak exertion. Given the non-clearly benign morphology of the BEVs, the symptomatic nature, and the uncertain family history of heart disease, further investigation with a cardiac MRI was performed, revealing a mildly dilated and hypokinetic left ventricle (EDV 106 ml/m2, EF 51%), and evidence of subepicardial-mesocardial fibrosis (LGE) of the left ventricle with a circumferential appearance; the right sections were normal. Based on these findings, we made diagnosis of Arrhythmogenic Left Ventricular Cardiomyopathy. Genetic testing revealed a heterozygous variant of the FLNC gene, presumably pathogenic (ACMG class 4). We decided for Implantation of ICD in primary prevention. The patient failed the subcutaneous ICD screening test due to ventricular undersensing related to low QRS voltages; therefore an extravascular ICD implantation was chosen. Pharmacological therapy with Ramipril 5 mg and Bisoprolol 2.5 mg was initiated. A defibrillator check revealed several rapid, non-sustained ventricular tachycardias (suspected torsades de pointes). A follow-up echocardiogram after three months of drug therapy revealed reverse remodeling of the left ventricle and normalization of left ventricular systolic function (biplane EF 61%).