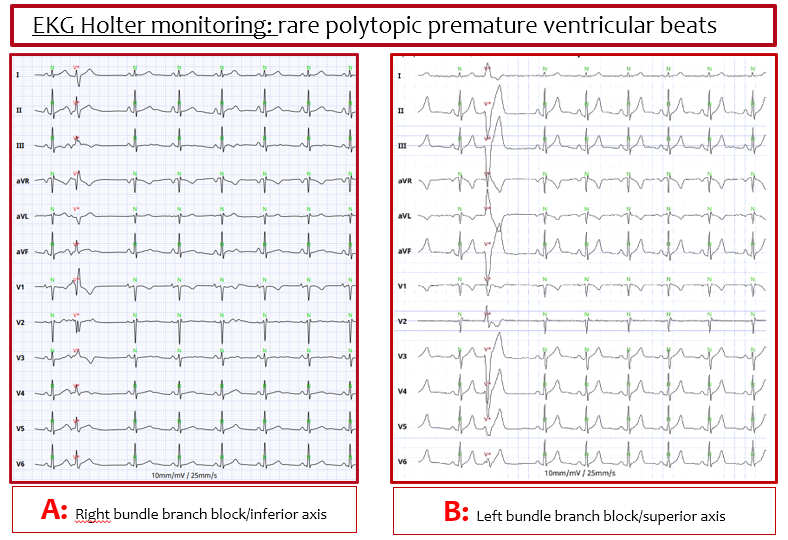
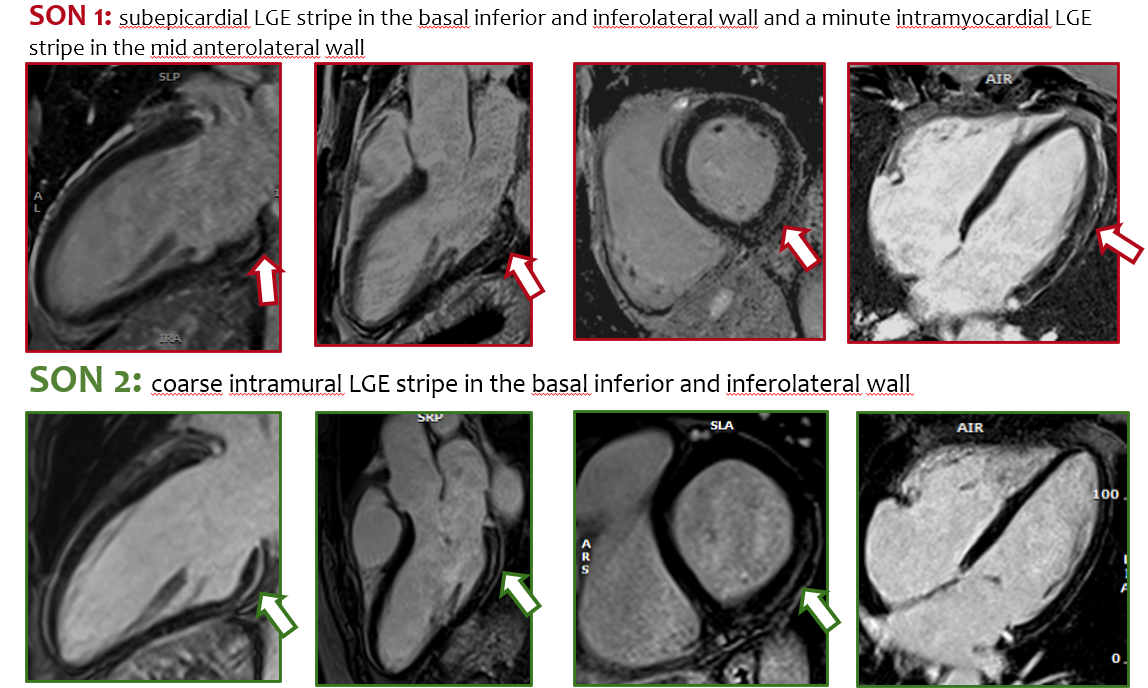
Background: Dilated cardiomyopathy (DCM) related to LMNA mutations is characterized by involvement of the atrioventricular (AV) conduction system, atrial arrhythmias and a high risk of malignant ventricular arrhythmias (MVA), even in the presence of mildly reduced or preserved left ventricular ejection fraction (LVEF). Case: We report a familial case of LMNA-related DCM involving a 70 years-old male proband and his two sons (aged 37 and 34 years), all carriers of heterozygous LMNA variant. The proband initially presented acute heart failure and atrial flutter. Significant coronary artery disease was excluded and CMR showed non-ischemic myocardial fibrosis, with intramural LGE stripe in the interventricular septum and basal posterior wall (LVEF 15%). An ICD was implanted and later upgraded to CRT-D. He subsequently experienced MVA, successfully terminated by a single shock, prompting genetic testing and family screening. Both sons, who were asymptomatic, underwent comprehensive evaluation with ECG, Holter monitoring, and exercise testing which showed no MVA (only rare polytopic premature ventricular beats, file 1), nor AV conduction disturbances. Echocardiogram was unremarkable. CMR showed non-ischemic myocardial fibrosis with preserved LVEF (file 2). The risk prediction score for VTA was low (<10%), so ICD implantation was deferred. Considering myocardial fibrosis and the dynamic arrhythmic risk, loop recorders were implanted and low-dose beta-blocker was initiated. Conclusion : In LMNA-related DCM, early electrical manifestations and myocardial fibrosis may precede overt systolic dysfunction. In asymptomatic mutation carriers, an individualized approach combining genetics, CMR tissue characterization, validated risk scores, and prolonged rhythm monitoring may enable more refined prognostic stratification and timely intervention.