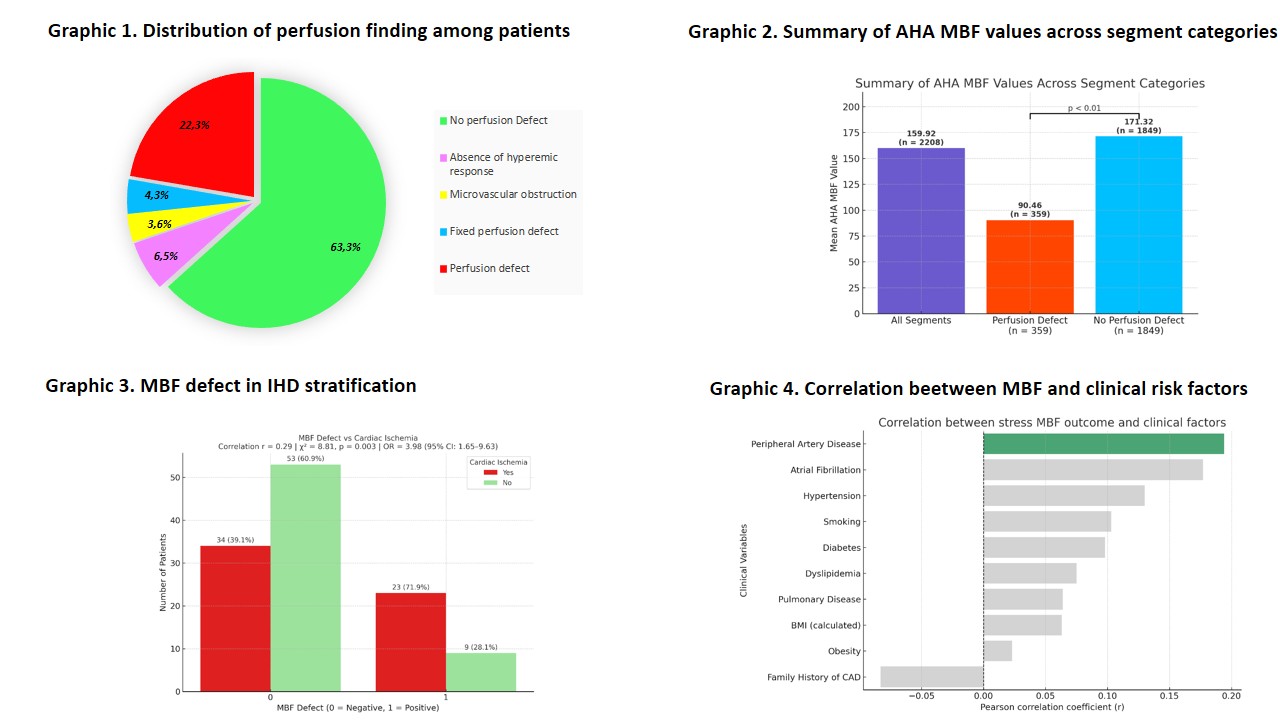
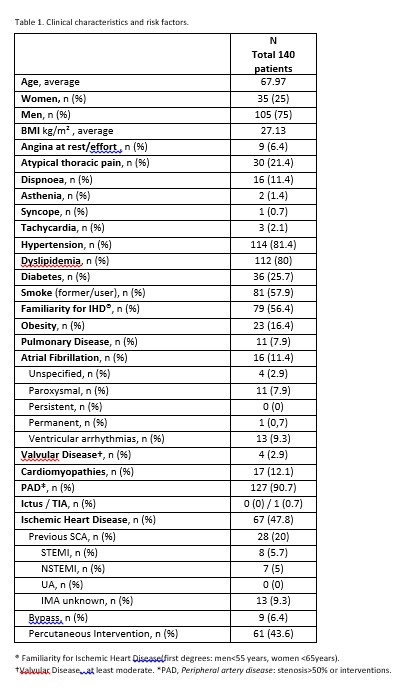
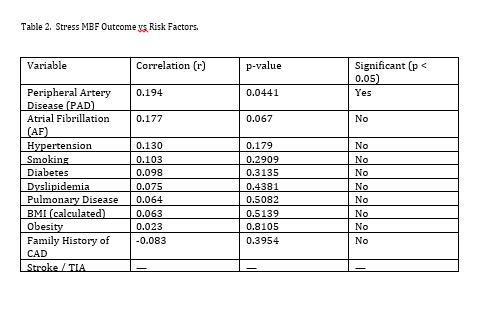
Stress Myocardial CT perfusion has emerged as a noninvasive modality for simultaneous anatomical and functional assessment of coronary artery disease, in a single scan session. This study investigates the relationship between MBF defects and main cardiovascular risk factors, providing reproducible thresholds that may distinguish normal from abnormal perfusion. Methods.A total of 140 patients (mean age 67.9±11.1 years; 75% men, Tab.1) were studied by stress myocardial CT perfusion (regadenoson). MBF stress response was classified as normal (MBF=0) or impaired (MBF=1).Patients were categorized based on MBF response [Graphic 1], risk factors and Ischemic Heart Disease (IHD) status for statistical analysis (Chi-squared analysis, Pearson correlation coefficient r and Odds Ratio). Results. The mean MBF across all AHA segments was 159.92 ml/100ml/min (n = 2208 segments).When stratified by perfusion status, segments with a perfusion defect showed a significantly lower mean MBF of 90.46 ml/100ml/min (n = 359, Graphic 1), compared to 171.32 ml/100ml/min (n = 1849) in segments without perfusion defects, with a significant difference (p < 0.01) [Graphic 2.].These results support the use of these MBF values as potential cut-offs. Stratifying patients based on the presence of known ischemic heart disease (IHD), a moderate positive correlation between MBF impairment and the presence of IHD (Pearson correlation coefficient r = 0.29; chi-squared test χ² = 8.81, p = 0.003) suggests that reduced MBF may be more associated with the presence of previous IHD [Graphic 3]. Furthermore, patients with an MBF defect were found to have a fourfold increased risk of having IHD [Odds Ratio (OR) 4.00, 95% C.I 1.57-10.2], suggesting that MBF impairment is a strong noninvasive marker of myocardial ischemia. Furthermore, the data suggest that CT perfusion has a diagnostic relevance in enhancing the likelihood of detecting ischemia in patients with established IHD. Regarding the main clinical risk factors, only Peripheral Artery Disease (PAD) showed a statistically significant correlation with MBF defect (r = 0.194, p = 0.044) [Tab 2., Graphic 4]. Conclusions.MBF impairment detected by CT stress perfusion is significantly associated with previous known IHD and PAD. According to our data, stress cardiac CT perfusion evaluation of MBF appears to be more effective in patients with pre-existing IHD and in those with PAD, representing population subgroups at higher risk for inducible ischemia.