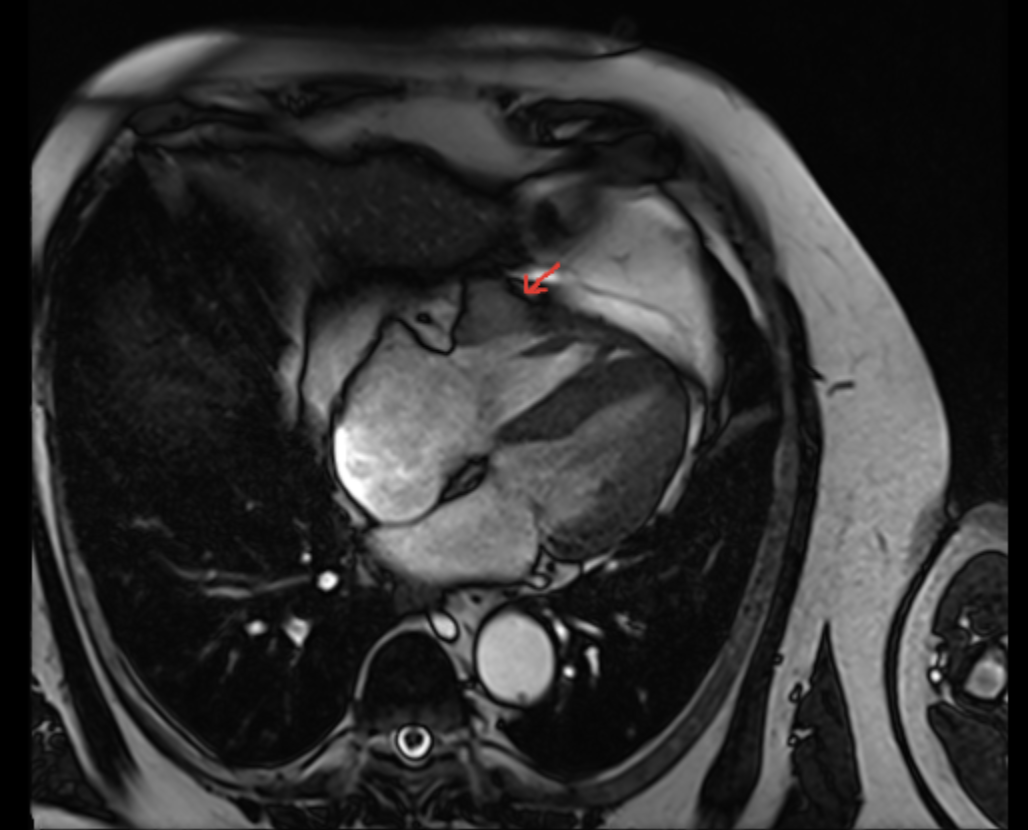
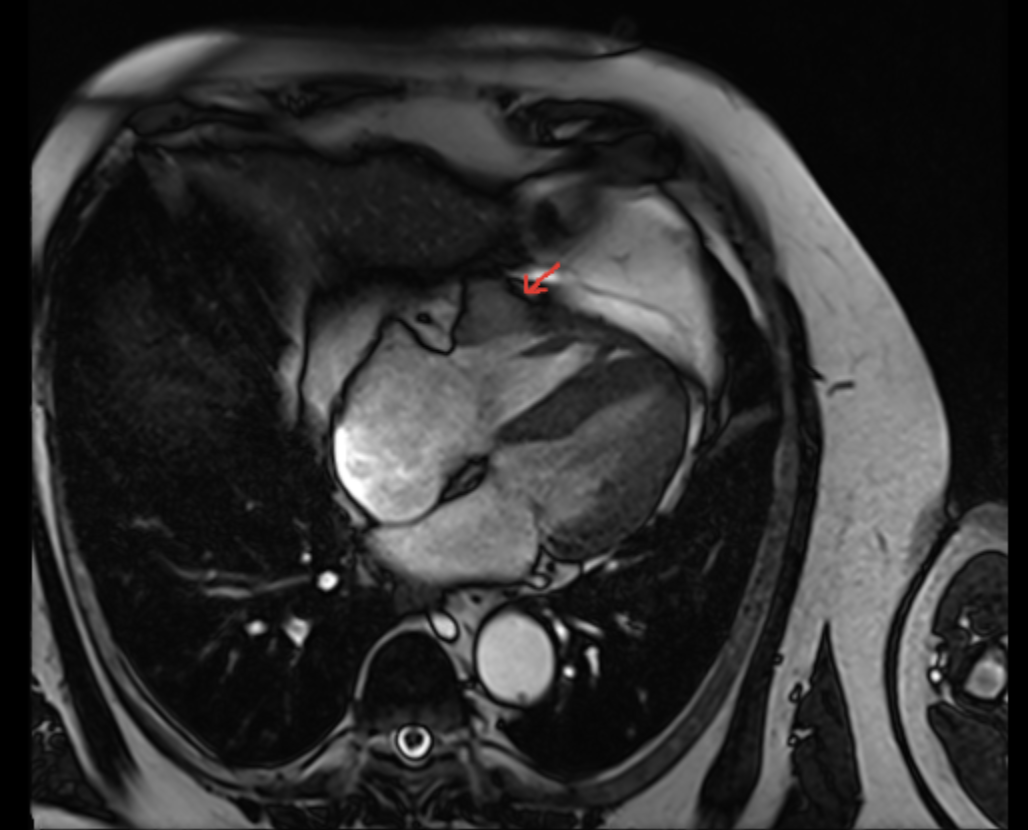
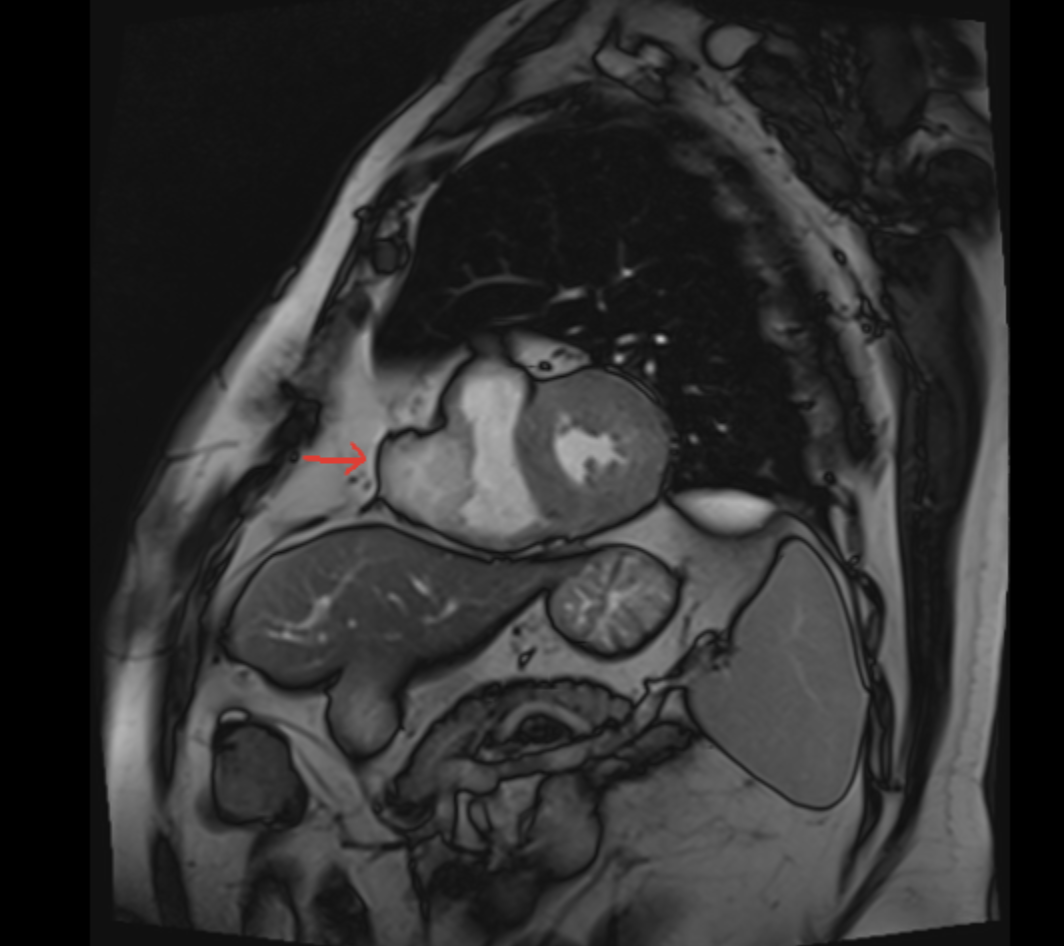
Introduction: Intracardiac metastasis from renal cell carcinoma (RCC) is an infrequent clinical finding. Immune checkpoint inhibitors (ICIs) have revolutionized cancer therapy but are associated with immune-related adverse events (irAEs). Among these, ICI-induced myocarditis is a rare but potentially fatal complication, typically occurring early after treatment initiation. However, vigilance must be maintained for delayed presentations, especially in complex oncological settings. Case Report: A 75-year-old male with a history of hypertension and previous left nephrectomy (2012) for RCC underwent surgical resection of a 38 mm right ventricular (RV) metastasis in early 2024. In April 2025, due to disease progression, he started combination therapy with Nivolumab and Cabozantinib (baseline LVEF 65%).In November 2025, after six months of therapy, routine oncological follow-up revealed a persistent, asymptomatic elevation of cardiac biomarkers (High-Sensitivity Troponin T 19.9 ng/ml, NT-proBNP 345 pg/ml, CK-MB 7.8 ng/ml). Echocardiography showed a significant decline in systolic function (LVEF 45%) and a reduction in RV longitudinal function (TAPSE 11 mm). To confirm the diagnosis and differentiate from post-surgical sequelae, Cardiac Magnetic Resonance (CMR) was performed. CMR quantitative tissue characterization revealed increased native T1 and T2 mapping values, along with a significantly elevated Extracellular Volume (ECV) fraction. Based on these findings, Nivolumab-induced myocarditis was diagnosed. Therapy was promptly interrupted and high-dose corticosteroid treatment was initiated, leading to clinical stabilization and a gradual downward trend of biomarkers. Conclusions: This case emphasizes the importance of cardiac monitoring during ICI therapy, even beyond the initial months of treatment. Delayed-onset myocarditis can present subclinically, with subtle biomarker elevations and biventricular dysfunction. A high clinical suspicion and the use of advanced CMR parameters, such as T1/T2 mapping and ECV, are essential for the timely diagnosis and management of this life-threatening irAE, particularly when prior cardiac surgery complicates the clinical picture.